
Introduction
Infant development represents one of the most dynamic and sensitive periods of human growth, encompassing rapid changes in physical, cognitive, social, and emotional domains. The early years of life are crucial for establishing the foundation for later intellectual and socio-emotional functioning. Understanding and measuring infant development are therefore vital both for identifying normal developmental trajectories and for detecting early deviations that might indicate developmental delays or disorders (Sarason & Sarason, 2005).
Among the most widely recognized tools for assessing early development are the Bayley Scales of Infant and Toddler Development (BSID) and the Gesell Developmental Schedule (GDS). These instruments provide clinicians, researchers, and educators with standardized, reliable methods to evaluate developmental milestones and guide intervention planning.
Read More: Theory of Development Moral Development
The Importance of Assessing Infant Development
Developmental assessment in infancy is crucial because early identification of delays allows for timely intervention, which can significantly improve developmental outcomes (Kapur, 1995). The brain’s neuroplasticity during early childhood offers a unique window during which targeted interventions can foster recovery or compensation for developmental lags. Moreover, standardized developmental assessments help differentiate between transient developmental variations and more stable patterns of delay (Davison, Neal, & Kring, 2004).
According to Barlow and Durand (1999), assessing early developmental milestones helps clinicians understand both quantitative and qualitative aspects of child growth, such as the rate of acquiring new skills and the integration of motor, cognitive, and social functions. Tools like the BSID and GDS have thus become indispensable for psychologists, pediatricians, and early intervention specialists.
Bayley Scales of Infant and Toddler Development (BSID)
The Bayley Scales were first developed by Nancy Bayley in 1969, with subsequent revisions in 1993 (Bayley-II), 2006 (Bayley-III), and most recently the Bayley-IV edition. The BSID was designed to provide a comprehensive assessment of developmental functioning from 1 to 42 months of age, encompassing multiple domains of development. The instrument is based on the assumption that early developmental performance predicts later cognitive and motor functioning, and that early assessment can guide educational and therapeutic planning (Anastasi & Urbina, 2005).

Bayley Scales of Infant and Toddler Development (BSID)
The BSID integrates both behavioral and cognitive frameworks of development. It emphasizes the role of learning, problem-solving, and environmental interaction in shaping early cognitive processes (Lezak, 1995).
Structure and Domains
The Bayley Scales typically consist of the following key subscales (Bayley-III version):
- Cognitive Scale – Measures sensorimotor development, problem-solving, and early concept formation.
- Language Scale – Divided into receptive and expressive communication subtests.
- Motor Scale – Assesses both fine and gross motor skills.
- Social-Emotional Scale – Evaluates emotional regulation and engagement (based on caregiver report).
- Adaptive Behavior Scale – Assesses practical, conceptual, and social skills necessary for everyday functioning.
Each subtest provides standardized scores, composite indexes, and percentile ranks. This multidimensional approach allows clinicians to identify specific areas of strength and weakness, offering a comprehensive developmental profile (Butcher, Mineka, & Hooley, 2014).
Administration and Scoring
The BSID is administered individually by a trained psychologist or clinician using standardized materials. The examiner presents tasks that increase in difficulty, observing the infant’s performance and recording whether each task is successfully completed. Parent questionnaires are also used for domains like social-emotional functioning (Anastasi & Urbina, 2005).
Scoring yields scaled scores for each subtest, which are then converted into composite scores. These composite scores are compared against age norms, allowing the identification of developmental delays or advanced performance.
Applications
The BSID is extensively used in:
- Clinical diagnosis of developmental delays, intellectual disabilities, and neurodevelopmental disorders such as autism spectrum disorder (ASD).
- Research, particularly longitudinal studies examining the effects of early environmental factors on cognitive outcomes.
- Early intervention programs, where it guides individualized educational and therapeutic strategies (Kapur, 1995).
For instance, children born prematurely or with low birth weight are often assessed using the BSID to monitor developmental progress and detect potential deficits early (Lezak, 1995).
Strengths and Limitations
The BSID is widely praised for its standardization, reliability, and comprehensiveness. It provides an empirically validated measure that is sensitive to subtle developmental differences. According to Wolman (1975), its structured format and clear scoring criteria enhance diagnostic accuracy.
However, the BSID also faces criticism for being time-consuming and requiring specialized training. Cultural and socioeconomic factors can influence test performance, as many test items reflect Western norms of development (Carson, Butcher, Mineka, & Hooley, 2007). Moreover, while early scores may correlate with later development, predictive validity decreases as children grow older due to environmental influences and differential rates of development (Sarason & Sarason, 2005).
2. Gesell Developmental Schedule (GDS)
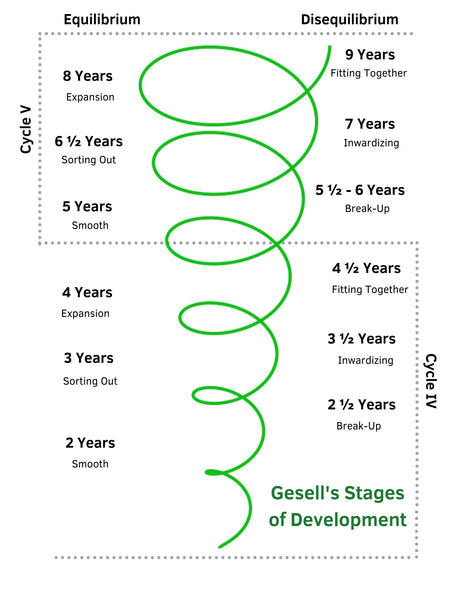
The Gesell Developmental Schedule, developed by Arnold Gesell in the early 20th century, was among the first systematic tools to evaluate infant and child development. Gesell, a pioneering developmental psychologist, emphasized that growth unfolds in a biologically predetermined sequence, influenced by both heredity and environmental factors (Rychlak, 1973). The GDS is rooted in the maturational theory, which views development as a natural progression following a predictable timetable.
Gesell Developmental Schedule
Structure and Domains
The Gesell Schedule assesses development across several key domains:
- Motor Behavior – Gross and fine motor coordination.
- Adaptive Behavior – Problem-solving and adaptability to new situations.
- Language Development – Comprehension and expressive skills.
- Personal-Social Behavior – Interactions with caregivers and peers.
Each domain yields a Developmental Quotient (DQ), calculated by dividing the developmental age by chronological age and multiplying by 100. This allows comparison across different domains and identification of areas of delay (Kellerman & Burry, 1981).
Administration and Scoring
The GDS involves direct observation and interaction with the child, often supplemented by caregiver interviews. Tasks are arranged according to age levels, and performance is noted as “passed” or “failed.” The examiner determines the developmental age by identifying the age level at which the child successfully completes a majority of items (Anastasi & Urbina, 2005).
Applications
The GDS has historically been used to:
- Screen for developmental delays and neurological impairments in infancy and early childhood.
- Monitor developmental progress in at-risk populations, such as children with low birth weight or genetic disorders.
- Support educational placement decisions in early childhood programs.
Its use in clinical and research settings has contributed significantly to understanding developmental norms and variability among young children (Kapur, 1995).
Strengths and Limitations
The GDS is valued for its simplicity, clinical utility, and observational nature. It allows for qualitative interpretation of a child’s behavior and developmental style, which can be particularly useful for early childhood educators and clinicians (Sundberg, Winebarger, & Taplin, 2002).
However, the test has limitations, including limited standardization and outdated norms that may not reflect contemporary developmental patterns (Sarason & Sarason, 2005). The focus on maturational sequences may also overlook cultural and environmental variability (Davison, Neal, & Kring, 2004). Despite these concerns, the GDS remains an influential tool in developmental assessment history and continues to inform modern test design.
Conclusion
The Bayley Scales of Infant and Toddler Development and the Gesell Developmental Schedule remain foundational tools in developmental psychology. While the Bayley Scales represent a modern, empirically validated approach to quantifying early development, the Gesell Schedule continues to offer valuable observational insights based on maturational theory. Both instruments contribute to the early detection of developmental challenges and the planning of interventions that support optimal growth during the formative years of life.
Understanding and appropriately applying these tools requires not only technical expertise but also sensitivity to cultural and contextual factors influencing child development. As research continues to advance, integrating standardized testing with dynamic and culturally responsive methods will remain essential for promoting healthy development in infancy and early childhood.
References
Anastasi, A., & Urbina, S. (2005). Psychological Testing (7th Ed.). Pearson Education: India.
Barlow, D.H., & Durand, V.M. (1999). Abnormal Psychology (2nd Ed.). Pacific Grove: Brooks/Cole.
Butcher, J.N., Mineka, S., & Hooley, J.M. (2014). Abnormal Psychology (15th Ed.). Dorling Kindersley (India) Pvt. Ltd.
Carson, R.C., Butcher, J.N., Mineka, S., & Hooley, J.M. (2007). Abnormal Psychology (13th Ed.). Pearson Education India.
Davison, G.C., Neal, J.M., & Kring, A.M. (2004). Abnormal Psychology (9th Ed.). New York: Wiley.
Kapur, M. (1995). Mental Health of Indian Children. Sage Publications: New Delhi.
Kellerman, H., & Burry, A. (1981). Handbook of Diagnostic Testing: Personality Analysis and Report Writing. New York: Grune & Stratton.
Lezak, M.D. (1995). Neuropsychological Assessment. Oxford University Press: New York.
Rychlak, F. (1973). Introduction to Personality and Psychopathology. Houghton Mifflin: New York.
Sarason, I.G., & Sarason, B.R. (2005). Abnormal Psychology. N.D.: Dorling Kindersley.
Sundberg, N.D., Winebarger, A.A., & Taplin, J.R. (2002). Clinical Psychology: Evolving Theory, Practice, and Research. Prentice-Hall: Upper Saddle River, N.J.
Wolman, B.B. (1975). Handbook of Clinical Psychology. New York: McGraw Hill.
Niwlikar, B. A. (2025, October 20). 2 Important Infant Development Measures. Careershodh. https://www.careershodh.com/infant-development-measures/