
Introduction
Neurodevelopmental disorders are a group of conditions characterized by early-onset impairments in cognitive, social, communicative, or behavioral development (American Psychiatric Association [APA], 2022). Accurate assessment of these disorders is critical for diagnosis, intervention planning, and monitoring outcomes. Standardized tools facilitate objective measurement of symptom severity and ensure comparability across clinicians and populations. In India and worldwide, several validated instruments are used to assess core features of disorders such as autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD).
Read More: Autism
The Indian Scale for Assessment of Autism (ISAA)
The Indian Scale for Assessment of Autism (ISAA) was developed by the National Institute for Mentally Handicapped (NIMH), Hyderabad, under the aegis of the Government of India’s Ministry of Social Justice and Empowerment (National Institute for Mentally Handicapped, 2009). The scale was designed to provide an indigenous, culturally appropriate tool for assessing autism in children and adults within the Indian population. Its development was motivated by the need for a standardized tool that reflected Indian social norms, linguistic diversity, and family structures, and that could support the certification of disability under the Rights of Persons with Disabilities Act.
Structure and Scoring
The ISAA consists of 40 items divided into six domains:
- Social relationship and reciprocity
- Emotional responsiveness
- Speech–language and communication
- Behavior patterns
- Sensory aspects
- Cognitive component and adaptive behavior
Each item is rated on a 5-point Likert scale from 1 (no abnormality) to 5 (severe abnormality). The total score categorizes the severity of autism into mild, moderate, or severe levels. The scale is based on both direct observation and caregiver interviews, and it is typically administered by trained clinicians, psychologists, or rehabilitation professionals.

ndian Scale for Assessment of Autism (ISAA) Scoring
Psychometric Properties
The ISAA has demonstrated satisfactory psychometric validity and reliability in multiple studies conducted in India. Patra et al. (2011) reported that ISAA showed high internal consistency (Cronbach’s alpha = 0.88) and good inter-rater reliability. Similarly, Chakraborty et al. (2015) found significant correlations between ISAA scores and clinical judgments of autism severity, supporting its construct validity. The tool has been used in epidemiological surveys and in diagnostic assessments at tertiary centers, establishing its utility for both clinical and research purposes.
Strengths
A major strength of ISAA lies in its cultural relevance. Many Western instruments may include items inappropriate for Indian socio-cultural contexts (e.g., expectations regarding eye contact or play behavior). ISAA’s items were developed using focus groups and field studies across diverse Indian regions, making it more sensitive to local behavioral norms (Chakraborty et al., 2015). Moreover, the tool aligns with Indian governmental requirements for disability certification, thereby integrating clinical assessment with policy and service delivery.
Limitations
Despite its advantages, ISAA is not without limitations. Critics note that the scale’s items may not fully align with contemporary DSM-5 criteria for Autism Spectrum Disorder (APA, 2022). Additionally, some items may show ceiling or floor effects in high-functioning or very young children (Patra et al., 2011). The need for trained raters and the potential for subjective bias in scoring are further limitations. Nonetheless, it remains one of the most practical and validated tools for autism assessment in India.
2. The Childhood Autism Rating Scale 2
The Childhood Autism Rating Scale (CARS), developed by Schopler, Reichler, and Renner in 1980, has been one of the most widely used observational tools for identifying autism and determining its severity. The Second Edition (CARS-2), revised by Schopler, Van Bourgondien, Wellman, and Love in 2010, incorporates changes to reflect evolving diagnostic criteria and to improve sensitivity across the autism spectrum (Schopler et al., 2010).
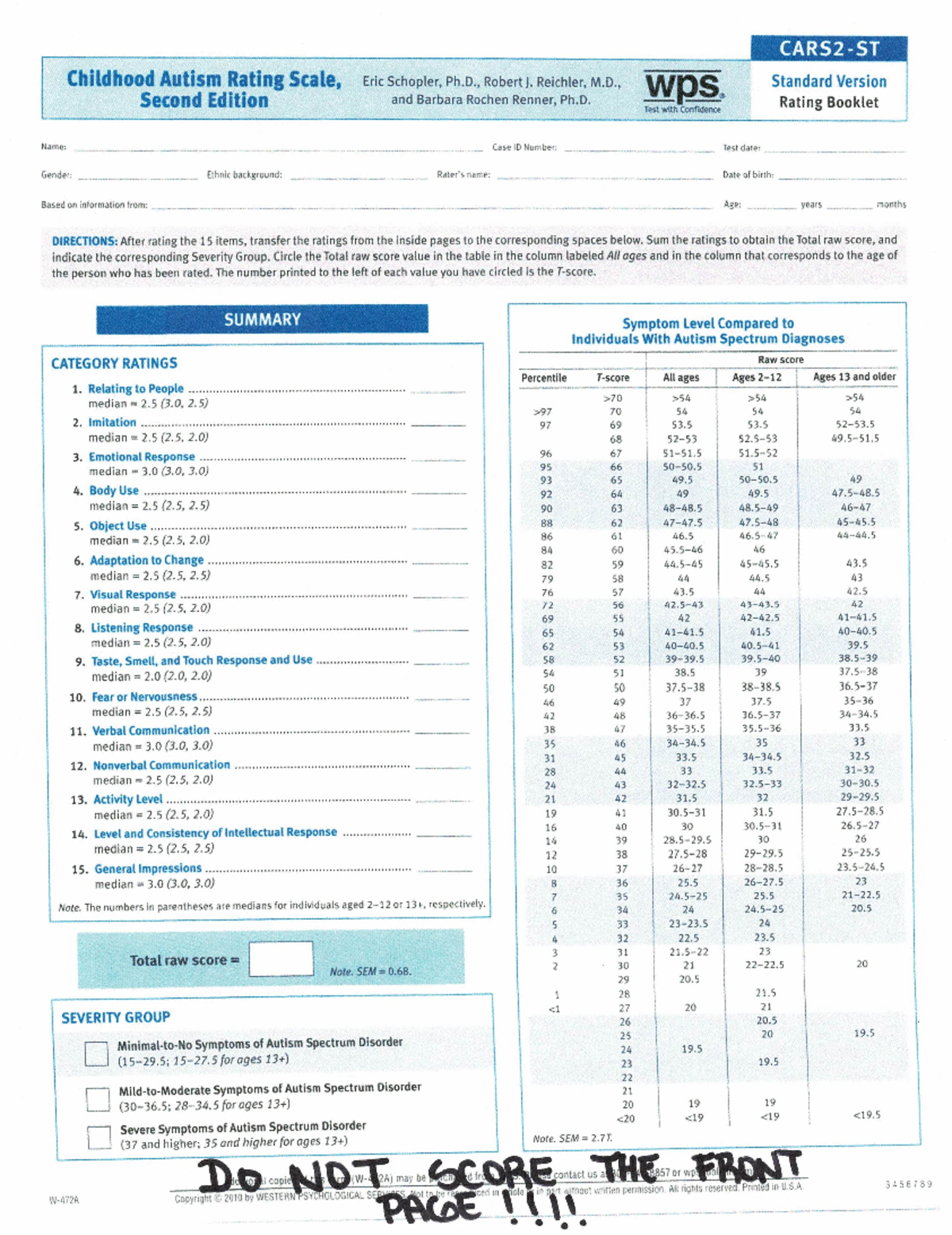
CARS 2
Structure and Administration
CARS-2 includes 15 items that evaluate a child’s behavior in areas such as relationships with people, emotional response, body use, adaptation to change, listening response, verbal and nonverbal communication, and intellectual functioning. Each item is rated on a 4-point scale from 1 (normal for age) to 4 (severely abnormal).
CARS-2 offers two versions:
- CARS-2 Standard Version (CARS2-ST): for children younger than six years or those with significant developmental delays.
- CARS-2 High Functioning Version (CARS2-HF): for children aged six years and above with average or higher intellectual functioning.
A Parent/Caregiver Questionnaire supplements clinical observation, enhancing reliability. Total scores categorize autism severity as minimal, mild-to-moderate, or severe.
Psychometric Properties
CARS-2 has been shown to have strong psychometric properties. Moulton et al. (2019) found high internal consistency (α = .91) and significant correlation with the Autism Diagnostic Observation Schedule (ADOS). Samadi, McConkey, and Kelly (2020) reported that CARS-2 demonstrated good discriminant validity and could reliably differentiate between autism and other developmental disorders across cultural contexts.
Because of its brevity and ease of use, CARS-2 remains a practical tool in both clinical and research settings, particularly where more resource-intensive assessments such as the ADOS are not feasible.
Strengths
CARS-2’s primary strengths are its brevity, ease of administration, and strong empirical support. It allows clinicians to quickly quantify autism severity and track changes over time. It is less time-consuming than structured diagnostic interviews, making it ideal for use in busy outpatient clinics or resource-limited settings (Schopler et al., 2010). Additionally, its revised version accommodates higher-functioning individuals, addressing a major limitation of the original CARS.
Limitations
CARS-2, however, depends heavily on clinician observation, which may introduce subjectivity. Differences in rater experience and training can lead to variability in scoring (Samadi et al., 2020). Furthermore, cultural factors can influence interpretation—for example, behaviors considered atypical in one culture may be normal in another. Hence, localized validation studies are recommended before use in new populations (Moulton et al., 2019).
Clinical Utility
CARS-2 is not a stand-alone diagnostic tool but a valuable component of a comprehensive autism assessment. It is often used alongside developmental history interviews, adaptive functioning scales, and cognitive testing. Its numeric severity index makes it useful for treatment planning and monitoring progress.
3. Adult ADHD Self-Report Scale (ASRS v1.1)
The Adult ADHD Self-Report Scale (ASRS) was developed by the World Health Organization (WHO) in collaboration with Kessler et al. (2005) as a screening tool for ADHD in adults. Historically, ADHD was regarded as a childhood disorder, but growing evidence indicates that symptoms persist into adulthood in approximately 60% of cases (Kessler et al., 2006). The ASRS was designed to provide a brief, standardized, and freely available screening instrument based on DSM-IV criteria for ADHD.

ASRS
Structure and Scoring
The ASRS v1.1 contains 18 items corresponding to DSM symptom criteria for ADHD, divided equally between inattention and hyperactivity–impulsivity domains. Each item is rated on a 5-point frequency scale (Never, Rarely, Sometimes, Often, Very Often).
The 6-item Part A screener is particularly valuable: endorsement of four or more shaded responses indicates symptoms highly consistent with ADHD and warrants further evaluation. Part B (12 items) provides additional detail for clinical assessment.
Psychometric Properties
The ASRS has demonstrated strong psychometric performance across multiple populations. Kessler et al. (2005) reported a sensitivity of 68.7% and specificity of 99.5% for the 6-item screener in detecting adult ADHD. Hines et al. (2012) and Gray et al. (2014) confirmed its good test–retest reliability and internal consistency (α > .80). The ASRS has also been validated in diverse cultural contexts, including Indian populations, showing robust correlations with clinician-administered ADHD diagnostic interviews (Bhatia & Nigam, 2019).
Strengths
The ASRS is efficient, easy to administer, and available in multiple languages. It is especially useful for screening large populations, primary care settings, or epidemiological studies (Kessler et al., 2006). Its self-report format empowers patients and provides insight into subjective experiences of inattention and impulsivity. Additionally, because it is based directly on DSM criteria, the ASRS aligns closely with clinical diagnostic frameworks.
Limitations
Despite its strengths, the ASRS should not be used in isolation for diagnosis. As a self-report measure, it is subject to bias from over- or under-reporting of symptoms, particularly in individuals with poor insight or comorbid psychiatric conditions such as anxiety or depression (Hines et al., 2012). Moreover, the ASRS may not distinguish ADHD symptoms from other disorders that impair attention or impulse control. Thus, positive screenings must be followed by a structured clinical interview and collateral information from family or workplace sources.
Clinical Application
The ASRS serves as a screening tool, not a diagnostic instrument. When used appropriately, it guides clinicians to identify adults who require comprehensive evaluation. It complements clinical interviews, neuropsychological testing, and functional assessments, enabling early identification and treatment initiation.
Conclusion
Accurate and culturally sensitive assessment tools are central to identifying neurodevelopmental disorders and tailoring appropriate interventions. The ISAA, CARS-2, and ASRS provide clinicians with structured frameworks to evaluate autism and ADHD across developmental stages. Each instrument has demonstrated reliability and validity within its target population. While ISAA emphasizes cultural and policy relevance for India, CARS-2 delivers an efficient and empirically supported international standard for autism assessment, and ASRS extends standardized evaluation to adult ADHD.
Effective assessment, however, requires integrating these tools with clinical judgment, developmental history, and multidisciplinary evaluation. Continued research into localization, standardization, and longitudinal application of such instruments will further strengthen their clinical utility and improve outcomes for individuals with neurodevelopmental disorders.
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). Washington, DC: Author.
Bhatia, M. S., & Nigam, V. R. (2019). Validation of the Adult ADHD Self-Report Scale (ASRS) in an Indian clinical sample. Indian Journal of Psychological Medicine, 41(2), 122–129.
Chakraborty, S., Thomas, P., Bhatia, T., & Varma, V. K. (2015). Assessment of severity of autism using the Indian Scale for Assessment of Autism (ISAA). Indian Journal of Psychological Medicine, 37(2), 169–174.
Gray, S., Woltering, S., Mawjee, K., & Tannock, R. (2014). The Adult ADHD Self‐Report Scale (ASRS): Utility in college students with attention‐deficit/hyperactivity disorder. Journal of Attention Disorders, 18(5), 412–420.
Hines, J. L., King, T. S., & Curry, W. J. (2012). The Adult ADHD Self-Report Scale for screening for adult attention deficit–hyperactivity disorder (ADHD). Journal of the American Board of Family Medicine, 25(6), 847–853.
Kessler, R. C., Adler, L., Ames, M., Barkley, R. A., Birnbaum, H., Greenhill, L., … & Ustun, T. B. (2005). The World Health Organization Adult ADHD Self-Report Scale (ASRS): A short screening scale for use in the general population. Psychological Medicine, 35(2), 245–256.
Kessler, R. C., Adler, L., Barkley, R., Biederman, J., Conners, C. K., Demler, O., … & Ustun, T. B. (2006). The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. American Journal of Psychiatry, 163(4), 716–723.
Moulton, E., Barton, M. L., Robins, D. L., Abrams, D. N., & Fein, D. (2019). Factor analysis of the Childhood Autism Rating Scale in a sample of two-year-old children with autism spectrum disorder. Autism, 23(3), 734–742.
National Institute for Mentally Handicapped. (2009). Indian Scale for Assessment of Autism (ISAA): Manual. Hyderabad: NIMH.
Patra, S., Arun, P., & Chavan, B. S. (2011). Use of the Indian Scale for Assessment of Autism (ISAA) in child guidance clinic: A report from north India. Indian Journal of Medical Research, 134(4), 522–527.
Samadi, S. A., McConkey, R., & Kelly, G. (2020). The psychometric properties of the Childhood Autism Rating Scale in a sample of Iranian children. Research in Autism Spectrum Disorders, 74, 101557.
Schopler, E., Van Bourgondien, M. E., Wellman, G. J., & Love, S. R. (2010). Childhood Autism Rating Scale, Second Edition (CARS-2). Los Angeles, CA: Western Psychological Services.
Niwlikar, B. A. (2025, October 22). 4 Important Assessment for Neurodevelopmental Disorders. Careershodh. https://www.careershodh.com/assessment-for-neurodevelopmental-disorders/