
Introduction
The assessment of personality is a cornerstone of clinical psychology, offering insight into an individual’s enduring patterns of thinking, feeling, and behaving (Sarason & Sarason, 2005). Personality inventories provide standardized methods for quantifying psychological characteristics, aiding in diagnosis, treatment planning, and research. Among the most influential and empirically validated tools are the Minnesota Multiphasic Personality Inventory–3 (MMPI-3) and the Millon Clinical Multiaxial Inventory–IV (MCMI-IV).
These instruments represent different theoretical traditions: the MMPI-3 emphasizes empirical criterion-keying, while the MCMI-IV is rooted in Theodore Millon’s theory of personality and psychopathology. Together, they provide clinicians with comprehensive frameworks for assessing both normal and maladaptive personality functioning.
Read More: DSM vs ICD
The Minnesota Multiphasic Personality Inventory–3 (MMPI-3)
The MMPI was originally developed by Hathaway and McKinley in 1943 as an objective tool for identifying psychiatric disorders. It employed an empirical keying approach—selecting items that differentiated between psychiatric and non-psychiatric populations (Kaplan, Sadock, & Grebb, 1994).

MMPI-2 vs MMPI-3
Subsequent revisions, including the MMPI-2 and MMPI-2-RF, addressed limitations such as outdated norms and item redundancy. The MMPI-3, released in 2020, represents the most recent and refined version, updating content to reflect modern language, cultural inclusivity, and contemporary diagnostic standards (Butcher, Mineka, & Hooley, 2014).
Structure and Scales
The MMPI-3 consists of 335 true-false items and yields multiple scale types:
- Validity Scales: Assess response consistency and honesty (e.g., VRIN-r, TRIN-r, F, L, K scales).
- Higher-Order Scales: Measure broad domains such as emotional/internalizing dysfunction, thought dysfunction, and behavioral/externalizing dysfunction.
- Restructured Clinical (RC) Scales: Provide refined measures of major psychopathology, reducing interscale overlap.
- Specific Problem Scales: Assess targeted domains like anxiety, anger, and family conflict.
- Personality Psychopathology Five (PSY-5) Scales: Parallel the Big Five model, assessing traits like negative emotionality and disconstraint (Davison, Neal, & Kring, 2004).
The scales were standardized on a normative sample reflecting U.S. Census demographics, enhancing cultural generalizability and interpretive accuracy (Anastasi & Urbina, 2005).
Administration and Scoring
The MMPI-3 can be administered via paper-pencil or computer-based formats. Administration requires approximately 35–50 minutes, depending on reading proficiency.
Scoring is automated, with T-scores (mean = 50, SD = 10) used to interpret results. Elevated scores (>65T) indicate potential clinical significance, while low or normal scores suggest adaptive functioning (Carson et al., 2007).
Critical attention must be given to validity indices; for example:
- High F scale → possible exaggeration or distress.
- Elevated K scale → defensiveness or denial.
- High VRIN/TRIN → inconsistent response patterns.
Interpretation
Interpretation of MMPI-3 results follows a multi-level process:
- Evaluate validity scales to ensure data reliability.
- Examine profile patterns across clinical scales to identify dominant traits or disorders.
- Analyze content and supplementary scales for contextual understanding (Sarason & Sarason, 2005).
Profiles may suggest specific syndromes (e.g., depression, paranoia) or personality styles (e.g., passive-aggressive, dependent). Interpretation should always integrate clinical interview data and behavioral observations for comprehensive assessment (Davison et al., 2004).
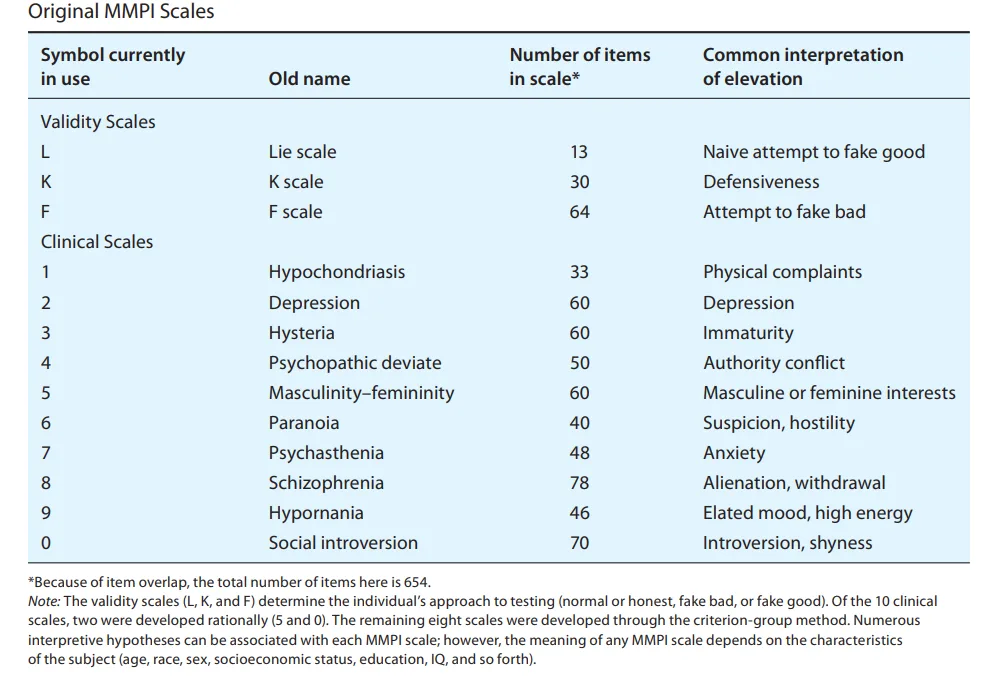
MMPI Scales
Applications
The MMPI-3 is widely used in:
- Clinical diagnosis: Differentiating between mood, psychotic, and personality disorders.
- Forensic evaluation: Assessing malingering, competency, and risk.
- Occupational and medical settings: Screening for stress resilience or somatic symptom tendencies.
- Research: Studying personality correlates of psychopathology and treatment response (Sundberg, Winebarger, & Taplin, 2002).
Read More: MMPI
Millon Clinical Multiaxial Inventory–IV (MCMI-IV)
The Millon Clinical Multiaxial Inventory–IV (MCMI-IV), developed by Theodore Millon, integrates a theoretical model of personality with clinical diagnosis. Unlike the MMPI-3, which is empirically derived, the MCMI-IV is theory-driven, grounded in Millon’s biosocial learning model and evolutionary theory (Rychlak, 1973; Kellerman & Burry, 1981).
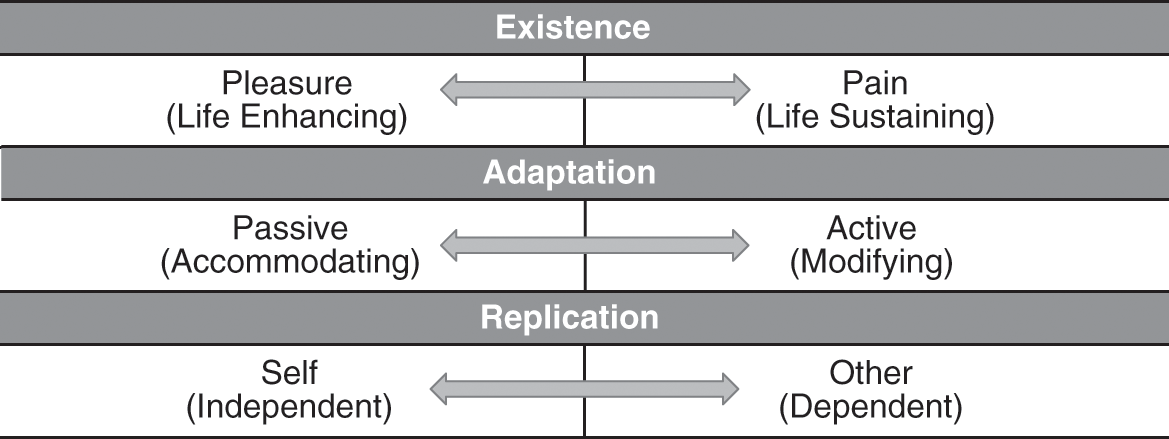
MCMI Drives
Millon viewed personality patterns as adaptive systems shaped by evolutionary drives (existence, adaptation, replication) and environmental interactions. Psychopathology results from maladaptive expressions of these drives.
Structure and Content
The MCMI-IV contains 195 true-false items, yielding 15 personality pattern scales, 10 clinical syndrome scales, and validity indices.
- Personality Pattern Scales: Correspond to DSM-5 personality disorders (e.g., Schizoid, Avoidant, Narcissistic, Borderline).
- Clinical Syndrome Scales: Assess acute disorders such as Anxiety, Bipolar Spectrum, and PTSD.
- Modifying Indices: Evaluate response tendencies (e.g., disclosure, desirability, debasement).
Each scale provides Base Rate (BR) scores rather than T-scores, aligning results with DSM-5 diagnostic thresholds (Carson et al., 2007).
Administration and Scoring
The MCMI-IV requires 25–30 minutes to administer, making it shorter and more focused than the MMPI-3.
Scores are automatically converted to Base Rate (BR) values:
- BR ≥ 75: Prominent personality traits
- BR ≥ 85: Likely personality disorder
Clinicians interpret patterns across personality and syndrome scales, noting which styles predominate or interact maladaptively (Anastasi & Urbina, 2005).
Interpretation Framework
Millon proposed that personality styles exist along a continuum of adaptiveness. Interpretation integrates:
- Structural traits: Core personality patterns.
- Functional traits: Behavioral expressions under stress.
- Dynamic interactions: How personality and symptoms reinforce each other.
For instance:
- Avoidant–Depressive Pattern: Characterized by sensitivity, pessimism, and social inhibition.
- Narcissistic–Antisocial Pattern: Reflects entitlement, exploitation, and lack of empathy (Sarason & Sarason, 2005).
Profiles often reveal comorbidities (e.g., Borderline + Depressive), aiding treatment planning and prognosis evaluation.
Conclusion
Personality inventories like the MMPI-3 and MCMI-IV remain foundational in modern psychological assessment. Each provides unique insights—MMPI-3 through its empirical validity and broad scope, and MCMI-IV through its theoretical precision and diagnostic specificity.
When used together, these tools help clinicians understand the complex interplay of personality structure, emotional regulation, and psychopathology. As emphasized by Sarason and Sarason (2005), accurate personality assessment enhances both diagnosis and treatment, allowing psychology to move closer to individualized, evidence-based care.
References
Anastasi, A., & Urbina, S. (2005). Psychological Testing (7th ed.). Pearson Education: India.
Barlow, D. H., & Durand, V. M. (1999). Abnormal Psychology (2nd ed.). Pacific Grove: Brooks/Cole.
Brannon, L., & Feist, J. (2007). Introduction to Health Psychology. Thomson Wadsworth: Singapore.
Butcher, J. N., Mineka, S., & Hooley, J. M. (2014). Abnormal Psychology (15th ed.). Dorling Kindersley (India) Pvt. Ltd: Pearson Education.
Carson, R. C., Butcher, J. N., Mineka, S., & Hooley, J. M. (2007). Abnormal Psychology (13th ed.). Pearson Education India.
Davison, G. C., Neal, J. M., & Kring, A. M. (2004). Abnormal Psychology (9th ed.). New York: Wiley.
Kaplan, H. I., Sadock, B. J., & Grebb, J. A. (1994). Kaplan and Sadock’s Synopsis of Psychiatry (7th ed.). B. I. Waverly Pvt. Ltd: New Delhi.
Kapur, M. (1995). Mental Health of Indian Children. Sage Publications: New Delhi.
Kellerman, H., & Burry, A. (1981). Handbook of Diagnostic Testing: Personality Analysis and Report Writing. Grune & Stratton: New York.
Lezak, M. D. (1995). Neuropsychological Assessment. Oxford University Press: New York.
Rychlak, F. (1973). Introduction to Personality and Psychopathology. Houghton Mifflin: New York.
Sarason, I. G., & Sarason, B. R. (2005). Abnormal Psychology. Dorling Kindersley: New Delhi.
Sundberg, N. D., Winebarger, A. A., & Taplin, J. R. (2002). Clinical Psychology: Evolving Theory, Practice, and Research. Prentice-Hall: Upper Saddle River, N.J.
Taylor, S. (2006). Health Psychology. Tata McGraw-Hill: New Delhi.
Niwlikar, B. A. (2025, October 14). 2 Important Personality Inventories: MMPI-3 and MCMI-IV. Careershodh. https://www.careershodh.com/mmpi-3-and-mcmi-iv/