
Introduction
Neuropsychological rehabilitation stands at the intersection of neuroscience, psychology, and functional therapy. It is a systematic and patient-centered process intended to help individuals regain as much of their cognitive, emotional, and behavioral functioning as possible following a neurological insult. This process is rarely linear, as recovery trajectories vary widely among individuals based on injury severity, age, premorbid functioning, and psychosocial factors.
Unlike traditional medical or physical rehabilitation, neuropsychological rehabilitation addresses “invisible” impairments—such as problems with memory, attention, emotional control, and decision-making—which may significantly hinder daily life despite an intact physical appearance. Given its complexity and scope, neuropsychological rehabilitation demands a highly individualized and interdisciplinary approach (Wilson, 2009).
Read More- Brain Hemisphere
Nature of Neuropsychological Rehabilitation
Neuropsychological rehabilitation is fundamentally multidimensional. It involves the assessment, treatment, and support of patients who experience impairments as a result of damage to the brain due to trauma, stroke, infections, tumors, or neurodegenerative diseases. It is concerned not only with the restoration of lost abilities but also with developing compensatory strategies and facilitating psychological adaptation to chronic disability.
This field is inherently collaborative, requiring the expertise of clinical neuropsychologists, speech and language therapists, occupational therapists, physiotherapists, psychiatrists, social workers, and educators. Together, these professionals create an integrated treatment plan tailored to the individual’s needs (Prigatano, 1999).
Importantly, rehabilitation is not always about achieving a complete return to previous levels of functioning. It often involves helping individuals adapt to a new way of life, using their existing strengths to overcome or work around deficits. This focus on empowerment and autonomy is central to the ethos of neuropsychological rehabilitation.
Goals of Neuropsychological Rehabilitation
The goals of neuropsychological rehabilitation are multifaceted and patient-centered, reflecting the complex and individualized consequences of neurological injury or illness. They aim not just at symptom reduction but at functional recovery and psychosocial well-being. These goals can be broadly categorized into four interrelated domains:

Principles of Neuropsychological Rehabilitation
1. Restoration of Cognitive Function
A cornerstone of neuropsychological rehabilitation is the restoration of disrupted cognitive abilities. This process is underpinned by the concept of neuroplasticity, the brain’s capacity to reorganize and form new neural connections following injury.
- Targeted cognitive exercises—including attention drills, memory recall tasks, language comprehension activities, and problem-solving scenarios—are designed to stimulate damaged regions of the brain.
- Computer-assisted cognitive training programs can personalize difficulty levels and track progress over time, offering adaptive feedback that reinforces learning.
- For instance, in individuals recovering from stroke-induced aphasia, structured language exercises may help reacquire naming and fluency skills, while those with attention deficits post-TBI may engage in tasks to increase sustained and selective attention.
It’s important to note that full restoration may not always be achievable, especially in progressive or severe conditions. Nonetheless, even partial improvements can significantly impact quality of life and daily function.
2. Compensation and Strategy Training
When certain cognitive functions are irreversibly impaired, the focus shifts from restoration to compensation. The goal is to help individuals adapt to their limitations using tools and strategies that enhance functioning in real-world settings.
Internal strategies include cognitive techniques such as:
- Mnemonics: Associative memory tools that link new information to familiar concepts.
- Self-instructional training: Encouraging individuals to verbalize steps aloud as they perform tasks.
- Visualization and mental rehearsal: Strengthening memory through mental imagery.
External strategies involve environmental modifications or assistive tools:
- Notebooks or memory diaries for recording appointments and tasks.
- Electronic devices such as smartphones with alarms, calendars, and GPS apps.
- Sticky notes, whiteboards, or color-coded labels as visual reminders.
These strategies are particularly critical for conditions like dementia, chronic TBI, or executive function disorders, where deficits persist despite targeted therapy. Teaching individuals to integrate these tools into their daily routines empowers them to regain autonomy.
3. Psychological and Emotional Adjustment
Neuropsychological injuries often affect not only cognition but also mood, personality, and emotional resilience. Psychological reactions may include:
- Depression, often stemming from lost independence or perceived identity changes.
- Anxiety, particularly in relation to uncertainty about recovery or return to work.
- Irritability and emotional lability, resulting from disrupted brain circuits regulating mood.
Psychological rehabilitation plays a central role in helping individuals cope with these changes:
- Cognitive-behavioral therapy (CBT) can help restructure maladaptive thought patterns, enhance coping mechanisms, and build emotional regulation skills.
- Support groups and peer mentoring offer shared experiences, reduce isolation, and promote emotional validation.
- Psychoeducation enables patients and families to understand emotional consequences of brain injury, helping to normalize and manage reactions effectively.
The emotional adjustment process is gradual and deeply personal, often requiring long-term therapeutic engagement.
4. Reintegration and Independence
Ultimately, neuropsychological rehabilitation strives to support individuals in rejoining their communities and living meaningful, independent lives. This requires more than cognitive recovery—it involves social, vocational, and environmental adaptation.
Social reintegration may include retraining in communication skills, rebuilding relationships, and navigating public or group settings.
Vocational rehabilitation involves:
- Work readiness assessments
- Job coaching and placement support
- Workplace modifications (e.g., reduced hours, adapted roles)
Home independence includes resuming roles such as parenting, budgeting, cooking, or transportation with necessary support structures in place.
Clinicians often collaborate with social workers, occupational therapists, and vocational counselors to facilitate this transition, acknowledging that successful reintegration is a process that continues well beyond the clinic.
Theoretical Models in Neuropsychological Rehabilitation
Rehabilitation is not one-size-fits-all. Effective interventions are guided by theoretical models that provide a rationale for treatment and shape how recovery is pursued. These models offer diverse perspectives on how the brain heals and how people adapt to cognitive loss.
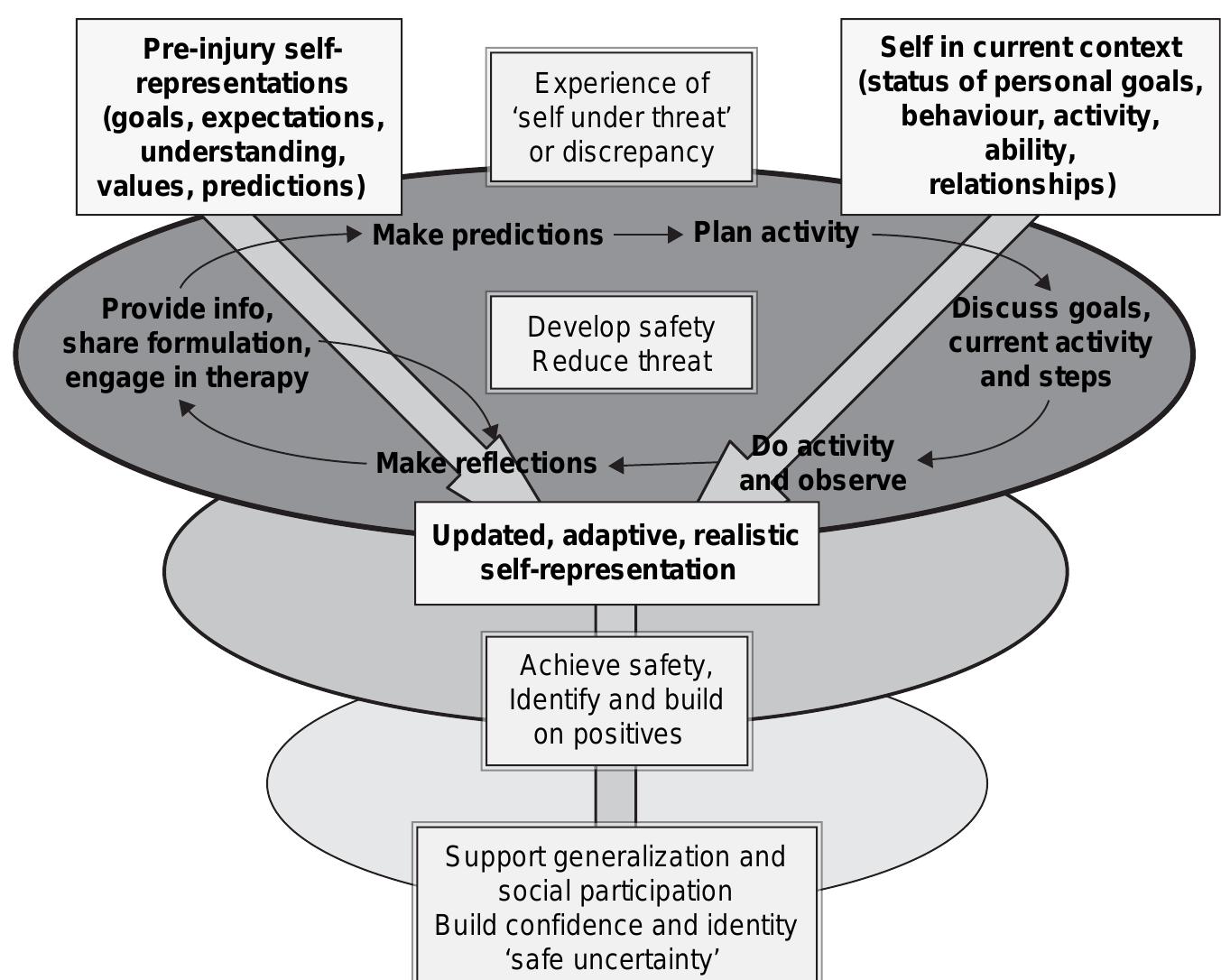
Neuropsychological Rehabilitation (Wilson et al)
1. Restorative Models
Restorative models focus on rebuilding lost functions by directly stimulating damaged cognitive systems. The underlying assumption is that with enough repetition and task specificity, neural pathways can be reactivated or restructured.
- For example, repetitive attention training (e.g., responding to visual or auditory cues) may help reactivate attentional networks in the parietal lobe.
- Language rehabilitation for aphasia might involve intensive naming drills, phoneme repetition, and reading tasks to stimulate perisylvian language areas.
Clinical research supports that these methods, when applied consistently and early post-injury, can lead to significant improvements, especially in mild-to-moderate brain injuries.
2. Compensatory Models
These models accept that some functions may be permanently lost and instead emphasize teaching the individual to work around the deficits.
- The goal is functionality, not necessarily full cognitive restoration.
- Real-world applications include:
- A person with executive dysfunction learning to use a detailed planner and daily checklists.
- A person with memory impairment using a smartphone voice assistant to create reminders.
Compensatory models are especially relevant in progressive conditions, such as Parkinson’s disease or Alzheimer’s, where the emphasis is on delaying functional decline and maximizing quality of life.
3. Contextualized or Ecological Models
Traditional cognitive tasks may not always transfer to real-world improvements. The ecological model, championed by researchers like Sohlberg and Mateer, advocates for training in meaningful, everyday environments.
Instead of training a memory skill through abstract word lists or computerized tasks alone, the ecological model recommends embedding the skill in daily routines—such as remembering a grocery list, following a cooking recipe, or navigating public transport. This approach enhances ecological validity, meaning the training is more likely to transfer to real-life use.
- Simulated real-world practice: Patients might rehearse using ATM machines, budgeting household expenses, or preparing meals as part of therapy.
- Role-specific tasks: For a parent, this might involve helping a child with homework, while for a professional, it could mean returning to job-related problem-solving.
This model aligns closely with client-centered rehabilitation, recognizing that relevance and personal meaning drive motivation and neurocognitive gains.
Components and Approaches in Rehabilitation
Effective neuropsychological rehabilitation is modular and integrative, combining multiple components tailored to the individual’s deficits, strengths, personality, and environment. Below is a deeper dive into key intervention types.
1. Cognitive Remediation
Cognitive Remediation Therapy (CRT) targets the recovery or enhancement of specific cognitive domains, including:
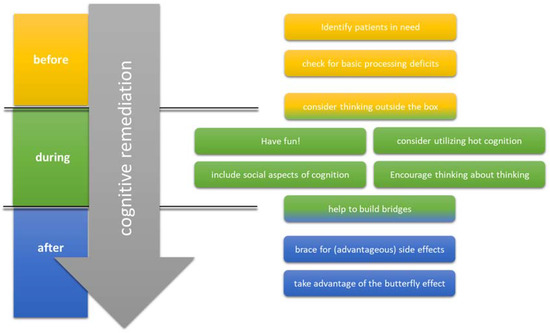
Cognitive Remediation
- Attention: Through exercises such as trail-making, visual scanning, and selective auditory focus tasks.
- Memory: Recalling stories, sequences, or paired associations; using spaced retrieval and errorless learning techniques.
- Executive Functions: Tasks requiring planning, response inhibition, decision-making, and cognitive flexibility (e.g., sorting, switching tasks, or solving multistep problems).
- Processing Speed: Timed reaction tasks or information-matching exercises to improve cognitive fluency.
Modern CRT often involves computerized platforms that adapt difficulty levels in real-time and provide feedback. These programs may be delivered in clinic, at home, or via tele-rehabilitation platforms.
Evidence base: Cicerone et al. (2011) reported that CRT, especially when embedded in broader rehabilitation plans, leads to improvements not only in test scores but also in functional outcomes such as independence, academic success, and workplace performance.
Importantly, CRT is most effective when paired with metacognitive training—teaching clients to monitor their own thinking and apply strategies across contexts.
2. Compensatory Strategies
Compensatory strategies are often the most practical and sustainable approach, especially for those with chronic impairments. These strategies are custom-designed to bypass specific cognitive barriers.
Internal Aids
- Verbal rehearsal: Repeating a name or fact several times to encode it better.
- Chunking: Grouping numbers or items into manageable units (e.g., breaking a phone number into segments).
- Visualization: Creating mental images or “mind maps” to anchor information.
- Self-talk and self-monitoring: Coaching oneself through tasks (“First I do this, then that…”).
External Aids
- Written tools: Journals, cue cards, calendars, sticky notes.
- Digital aids: Smartphone alarms, task management apps (e.g., Google Keep, Evernote), GPS navigation.
- Environmental modifications: Labeling drawers, creating “memory stations” at home for essential items like keys or medication.
Therapists not only introduce these tools but train clients in their consistent use, ensuring they become habitual and embedded into daily routines.
3. Psychological and Emotional Interventions
Cognitive and behavioral changes often lead to a secondary emotional crisis, which, if unaddressed, can hinder rehabilitation.
Cognitive-Behavioral Therapy (CBT)
CBT has been widely adapted for individuals with brain injuries:
- Modifying unhelpful thoughts: E.g., “I can’t do anything anymore” becomes “I can’t do everything I used to, but I’m learning to adapt.”
- Behavioral activation: Encouraging structured activity to combat apathy or depressive withdrawal.
- Cognitive restructuring: Helping individuals reframe their identity and future in a more realistic and hopeful way.
Mindfulness and Stress Management
Mindfulness practices have shown promise in improving emotional regulation and attentional control, especially in individuals with TBI, who often struggle with irritability or impulsivity.
- Breathing exercises, guided imagery, and progressive muscle relaxation are commonly used.
- Group-based interventions often blend these techniques with psychoeducation.
Family Education and Counseling
Family members may experience frustration, grief, or confusion regarding the patient’s behavior or prognosis.
- Psychoeducation sessions explain the neurobehavioral effects of injury (e.g., why impulsivity or forgetfulness occurs).
- Counseling supports the adjustment to new roles and expectations (e.g., caregiver, financial provider).
- Boundary-setting training ensures families encourage independence while providing support.
When family systems are integrated into the therapeutic process, patients often show greater adherence, fewer emotional outbursts, and better long-term outcomes.
4. Social and Vocational Skills Training
For many clients, especially younger individuals or working-age adults, regaining social competence and employment is a top priority. Neurological damage often impairs:
- Theory of Mind (understanding others’ perspectives)
- Non-verbal communication (e.g., reading facial expressions)
- Self-regulation in group dynamics or high-pressure environments
Social Skills Training
- Role-playing exercises simulate conversations, conflict resolution, or team interactions.
- Video feedback helps clients observe and refine their communication style.
- Group-based rehabilitation provides opportunities for peer interaction and feedback.
Vocational Rehabilitation
Returning to the workforce can dramatically improve self-esteem, financial security, and social connection.
- Work readiness assessments determine cognitive and emotional suitability for various roles.
- Supported employment programs place clients in actual work environments with job coaching, task simplification, and workplace accommodations.
- Educating employers about the nature of cognitive impairments helps foster inclusive workplaces.
In progressive conditions or severe injuries, the goal may shift from traditional employment to meaningful occupation, such as volunteering, part-time work, or creative hobbies that provide structure and identity.
Ethical and Cultural Considerations in Neuropsychological Rehabilitation
Ethical Considerations
Neuropsychological rehabilitation operates within a framework of ethical responsibility to the patient, family, and broader society. Key ethical issues include:
- Informed Consent: Individuals with cognitive impairments may lack the capacity to fully understand the nature and implications of their treatment. Clinicians must assess capacity carefully and involve legal guardians when necessary.
- Autonomy vs. Safety: A common ethical dilemma involves balancing the patient’s right to independence with the need to ensure safety. For example, a person with memory deficits may insist on living alone, despite the risks associated with forgetting medications or leaving appliances on.
- Resource Allocation: Given limited rehabilitation resources, prioritizing treatment for those most likely to benefit poses another ethical challenge. Equitable access should remain a guiding principle.
- Confidentiality and Family Involvement: Brain injuries often affect interpersonal relationships, necessitating collaboration with family members. Clinicians must navigate confidentiality while involving caregivers appropriately.
Cultural Sensitivity
Cultural background can profoundly influence how individuals perceive illness, recovery, disability, and therapy. For instance:
- In some cultures, mental health and cognitive dysfunction are stigmatized, which may deter individuals from seeking rehabilitation.
- Family dynamics, gender roles, and religious beliefs can shape expectations regarding caregiving, return to work, and independence.
Practitioners must adopt culturally competent approaches, including language translation services, culturally relevant psychoeducation, and community-based support systems to maximize treatment efficacy.
Interdisciplinary Collaboration
A defining characteristic of successful neuropsychological rehabilitation is a cohesive interdisciplinary team, each member contributing specialized knowledge to the collective goal of patient recovery.
Team Members and Their Roles
- Clinical Neuropsychologist: Assesses cognitive function and designs interventions targeting specific deficits.
- Occupational Therapist: Focuses on restoring daily living skills and functional independence.
- Speech-Language Pathologist: Addresses communication deficits, swallowing difficulties, and cognitive-communication disorders.
- Physiotherapist: Assists in physical mobility, balance, and coordination.
- Psychiatrist or Clinical Psychologist: Manages emotional and behavioral health through medication or psychotherapy.
- Social Worker and Case Manager: Facilitate access to services, housing, vocational training, and family support.
Integrated Care Plans
Weekly interdisciplinary meetings, progress reviews, and collaborative goal setting ensure that interventions are cohesive, relevant, and patient-centered. Shared decision-making between team members and the patient enhances adherence and outcomes.
The Role of Caregivers and Family Members
The journey of rehabilitation extends beyond the individual. Families and caregivers are integral, often serving as the primary source of daily support. However, the emotional and physical toll on caregivers is significant and often under-recognized.
Caregiver Burden
Caregivers may experience depression, burnout, financial strain, and disrupted relationships. Chronic stress without proper support can compromise the caregiver’s health and the patient’s recovery.
Interventions for Caregivers
- Education Programs: Help families understand brain injury, prognosis, and behavioral changes.
- Respite Services: Provide temporary relief to prevent burnout.
- Support Groups: Offer emotional validation and shared experiences.
- Skill Training: Teach caregivers how to assist with memory prompts, manage challenging behaviors, and use assistive technologies.
Including caregivers in the rehabilitation process—through joint therapy sessions, progress reviews, and skill-building—has been shown to improve outcomes for both the patient and the caregiver.
Conclusion
Neuropsychological rehabilitation is more than a clinical discipline—it is a pathway to restored dignity, independence, and identity. Whether it is a young adult recovering from a motorcycle accident, a stroke survivor relearning how to speak, or an elderly individual managing cognitive decline, neuropsychological rehabilitation offers tools and hope for renewed functionality and life participation.
This complex process draws on science, empathy, and innovation. Its success lies in the delicate orchestration of brain science, therapeutic skill, interdisciplinary collaboration, and personal resilience. As technology evolves and the healthcare landscape shifts toward greater inclusivity, the field is poised to break new ground in accessibility and personalization.
By addressing not only the mind but the entire ecosystem of the patient—including their families, communities, and cultural values—neuropsychological rehabilitation can fulfill its ultimate goal: to heal, empower, and transform lives.
References
Cicerone, K. D., Langenbahn, D. M., Braden, C., et al. (2011). Evidence-based cognitive rehabilitation: Updated review of the literature from 2003 through 2008. Archives of Physical Medicine and Rehabilitation, 92(4), 519–530.
Prigatano, G. P. (1999). Principles of neuropsychological rehabilitation. Oxford University Press.
Sohlberg, M. M., & Mateer, C. A. (2001). Cognitive rehabilitation: An integrative neuropsychological approach. Guilford Press.
Wilson, B. A. (2009). Memory rehabilitation: Integrating theory and practice. Guilford Press.
Niwlikar, B. A. (2025, June 27). Neuropsychological Rehabilitation and 4 Important Goals of It. Careershodh. https://www.careershodh.com/neuropsychological-rehabilitation/