
Introduction
Dissociative disorders are a group of psychological disorders characterized by disruption in the normally integrated functions of consciousness, memory, identity, emotion, perception, body representation, and behavior (APA, DSM-5, 2013). Dissociation serves as a defense mechanism, usually linked with overwhelming stress, trauma, or abuse, where the individual separates themselves psychologically from a painful reality. According to Butcher, Mineka and Hooley (2014), dissociative disorders involve alterations in personal identity or memory that are beyond ordinary forgetting and cause significant impairment in social and occupational functioning.
Dissociative Disorders
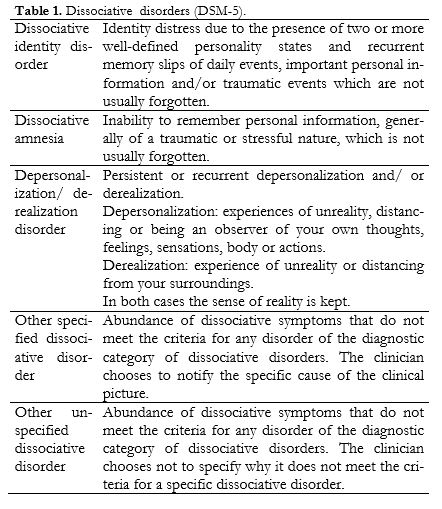
The DSM-5 (APA, 2013) places dissociative disorders under Trauma- and Stressor-Related conditions. The major forms include Dissociative Identity Disorder (DID), Dissociative Amnesia, Dissociative Fugue (now a specifier within Dissociative Amnesia), and Depersonalization/Derealization Disorder. These disorders are strongly associated with childhood trauma, long-term neglect, emotional or sexual abuse, and stress-related psychological conflict (Nevid, Rathus & Greene, 2014).
1. Dissociative Identity Disorder (DID)
Dissociative Identity Disorder, previously known as Multiple Personality Disorder, involves the presence of two or more distinct personality states, each with a unique pattern of perceiving, relating to and thinking about self and the world (APA, DSM-5, 2013). Individuals with DID experience amnesia for important personal information, and identity transitions may occur suddenly and can be accompanied by behavioral and physiological changes.
Dissociative Disorders
Features and Symptoms
According to DSM-5 (APA, 2013) and Barlow & Durand (2005), the major symptoms include:
- Two or more distinct identities or personality states
- Recurrent episodes of amnesia inconsistent with ordinary forgetting
- Gaps in recall for everyday events, traumatic events, or personal information
- Feeling controlled by internal voices or forces
- Sudden behavioral changes, change in handwriting or skills
- Derealization, depersonalization, and emotional numbness
- Anxiety, depression, self-harm, or suicidal behaviors
Butcher et al. (2014) emphasize that alternate personalities often differ in gender, age, name, tone of voice, and preferences, appearing to control behavior temporarily.
Etiology
- Trauma Model: Most theorists agree that DID develops due to chronic childhood trauma and abuse, particularly before age 6 (Alloy et al., 2005; Sarason & Sarason, 2002). Repeated trauma leads to dissociation as a survival strategy by mentally escaping harmful reality.
- Psychodynamic Perspective: Unconscious repression of intolerable memories results in fragmentation of identity (Carson, Butcher & Mineka, 2007).
- Cognitive-Behavioral View: Dissociation is reinforced because mentally escaping trauma reduces anxiety, creating learned avoidance patterns (Barlow & Durand, 2005).
- Sociocognitive Model: Some researchers argue DID results partly from therapist suggestion or cultural expectations (Butcher et al., 2014).
Treatment
There is no medication that cures DID; therapy is primary.
- Long-term psychotherapy to integrate identities (APA, 2013)
- Trauma-focused therapy
- Cognitive-behavioral therapy
- Hypnotherapy for memory recovery (controversial and used cautiously)
- Family education and support
- Medication only for comorbid anxiety or depression (SSRIs, antipsychotics)
2. Dissociative Amnesia
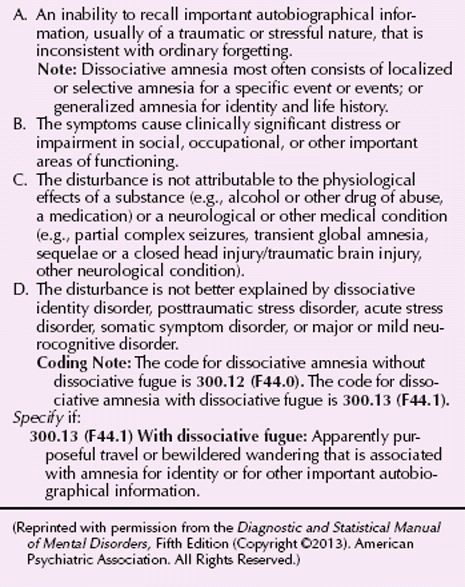
Dissociative Amnesia involves an inability to recall autobiographical information usually of a traumatic or stressful nature, inconsistent with ordinary forgetting (APA, DSM-5, 2013).
Types and Features
- Localized amnesia – failure to recall specific events
- Selective amnesia – recall of some but not all details
- Generalized amnesia – loss of memory for identity and life history
- Continuous amnesia – ongoing forgetting of new events
- Systematized amnesia – forgetting a specific category (e.g., about a person)
Symptoms include confusion, distress, anxiety, depression, and functional impairment (Nevid et al., 2014).
Etiology
- Severe trauma, natural disasters, accidents (Barlow & Durand, 2005)
- Military combat, abuse histories (Alloy et al., 2005)
- Psychological repression and self-protection (psychodynamic view)
Treatment
- Supportive psychotherapy
- Trauma-processing therapy
- Cognitive behavioral therapy
- Medication for comorbid anxiety
- Hypnosis or drug-assisted interviews (rarely used now)
3. Dissociative Fugue
Dissociative Fugue is sudden, unexpected travel away from home or workplace with inability to recall one’s past and confusion about identity (APA, DSM-5, 2013). The person may adopt a new identity and begin a new life for hours, days, or even months.
Symptoms
- Sudden travel away from familiar surroundings
- Inability to recall personal identity
- Sometimes a new identity formation
- Emotional numbness and confusion (Butcher et al., 2014)
Etiology
Highly associated with extreme stress such as disasters, war trauma, emotional shock, or loss (Carson et al., 2007).
Treatment
- Psycho-education and stress management
- Trauma therapy
- Hypnosis to recover memory
- CBT for coping skills
4. Depersonalization/Derealization Disorder
A dissociative disorder characterized by persistent or recurrent experiences of depersonalization (feeling detached from oneself) or derealization (feeling that surroundings are unreal) while reality testing remains intact (APA, DSM-5, 2013).
Symptoms
- Feeling like an outside observer of one’s body
- Emotional or physical numbness
- Perception of reality as dreamlike or distorted
- Loss of sense of time (Nevid et al., 2014)
Etiology
- Excessive stress and trauma
- Childhood emotional neglect (Sarason & Sarason, 2002)
- Anxiety and panic disorders
- Neurobiological dysregulation (Carson et al., 2007)
Treatment
- CBT to reduce catastrophic thinking
- Grounding techniques
- Mindfulness practices
- SSRI or anti-anxiety medications
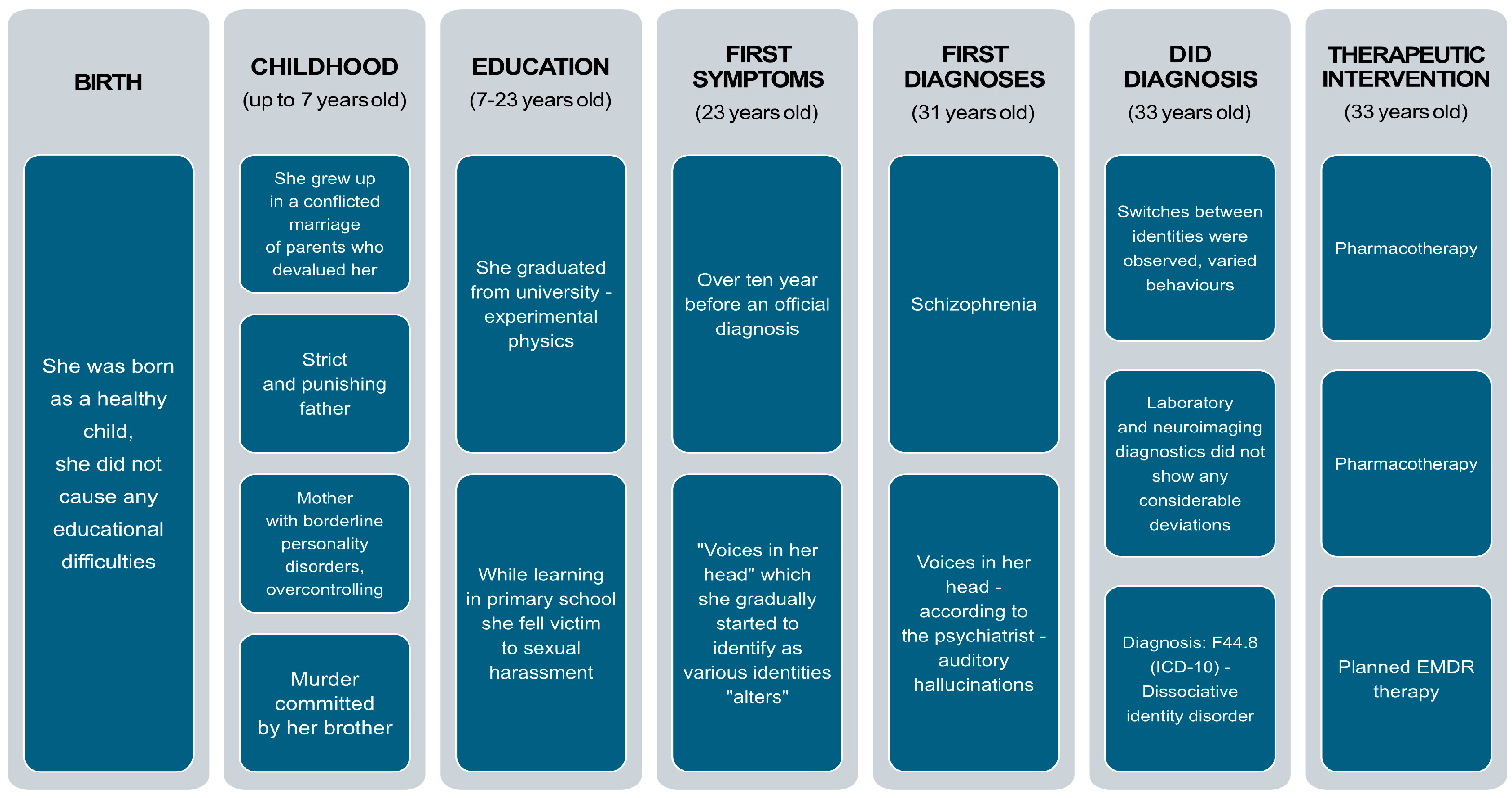
Dissociative Identity Disorder (DID) from a Psychodynamic Perspective
Conclusion
Dissociative disorders represent complex psychological responses to trauma and overwhelming stress, often rooted in childhood experiences. While symptom expression varies across disorders such as DID, Dissociative Amnesia, Fugue, and Depersonalization-Derealization disorder, they collectively reflect disruptions in memory, identity, and perception. With appropriate psychotherapeutic interventions, many individuals regain stability and functional recovery.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC.
Alloy, L. B., Riskind, J. H., & Manos, M. J. (2005). Abnormal Psychology: Current Perspectives (9th ed.). Tata McGraw-Hill.
Barlow, D. H. & Durand, V. M. (2005). Abnormal Psychology (4th ed.). Brooks/Cole Publishing.
Butcher, J. N., Mineka, S., & Hooley, J. M. (2014). Abnormal Psychology (15th ed.). Pearson Education.
Carson, R. C., Butcher, J. N., Mineka, S., & Hooley, J. M. (2007). Abnormal Psychology (13th ed.). Pearson Education.
Nevid, J. S., Rathus, S. A., & Greene, B. (2014). Abnormal Psychology (9th ed.). Pearson.
Sarason, I. G., & Sarason, R. B. (2002). Abnormal Psychology: The Problem of Maladaptive Behavior (10th ed.). Pearson Education.
Niwlikar, B. A. (2025, November 26). 4 Important Dissociative Disorders: Features, Etiology and Treatments. Careershodh. https://www.careershodh.com/dissociative-disorders/