
Introduction
Human sexuality is a central aspect of physical and emotional well-being. It involves biological processes, psychological experiences, relational dynamics, and sociocultural influences. When these factors function harmoniously, individuals typically experience fulfilling sexual responses. However, disturbances in any phase of the sexual response cycle can manifest as sexual dysfunctions—conditions characterized by impaired desire, arousal, orgasm, or sexual pain.
According to the DSM-5 (American Psychiatric Association, 2013), sexual dysfunctions involve clinically significant disturbances that cause marked distress and interpersonal strain. These conditions are common in both men and women and are influenced by physical health, mental health, relationship patterns, social norms, and cultural expectations. Authors such as Barlow & Durand (2005), Butcher, Mineka & Hooley (2014), and Carson et al. (2007) emphasize that sexual dysfunctions are multi-determined and rarely arise from a single cause.
Read More: Cognitive Therapy
The Human Sexual Response Cycle
The concept of the sexual cycle originates from the pioneering research of Masters and Johnson, later expanded by Kaplan. DSM-5 integrates these perspectives to describe sexual function along three core dimensions: desire, arousal, and orgasm.

Sexual Cycle
1. Desire Phase
Sexual desire (libido) includes:
- Sexual fantasies
- Interest in engaging in sexual activity
- Biological urges influenced by hormones, dopamine pathways, and psychological stimulation
Factors affecting desire:
- Hormonal fluctuations
- Stress and fatigue
- Body image
- Relationship satisfaction
- Mental health conditions
Low desire is one of the most commonly reported sexual difficulties.
2. Arousal Phase
Arousal includes both subjective feelings and physiological responses.
In males:
- Penile erection
- Increased testicular elevation
- Heightened sensitivity
In females:
- Vaginal lubrication
- Swelling of labia and clitoris
- Increased blood flow and muscle tension
General bodily changes include:
- Increased heart rate
- Respiratory changes
- Skin flush
Arousal disorders occur when these processes do not function adequately.
3. Orgasm Phase
Orgasm is characterized by:
- Peak sexual pleasure
- Rhythmic contractions of pelvic muscles
- Ejaculation in males
- Intense release of tension
Disorders involve delayed orgasm, absence of orgasm, or premature ejaculation.
4. Resolution Phase
After orgasm:
- Physiological arousal declines
- Muscles relax
- Heart rate stabilizes
- Men enter a refractory period (women generally do not)
Understanding the cycle helps clinicians identify which phase is impaired.
DSM-5 Classification of Sexual Dysfunction Disorders
DSM-5 requires symptoms to:
- Persist for at least 6 months
- Cause significant clinical distress
- Not be better explained by another disorder, medical condition, or substance use
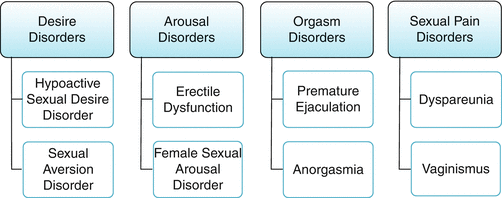
Sexual Dysfunction Disorder
The primary disorders include:
- Male Hypoactive Sexual Desire Disorder: Persistent low desire not attributable to normal aging or other factors.
- Female Sexual Interest/Arousal Disorder: Combined deficiencies in both desire and arousal.
- Erectile Disorder: Persistent difficulty attaining or maintaining an erection.
- Female Orgasmic Disorder: Marked delay or absence of orgasm despite adequate stimulation.
- Delayed Ejaculation: Delay or absence of ejaculation in most sexual encounters.
- Premature (Early) Ejaculation: Ejaculation occurring within approximately 1 minute of penetration or earlier than desired.
- Genito-Pelvic Pain/Penetration Disorder: Includes: pain during intercourse, fear or anxiety about pain, pelvic floor tightness, and difficulty with penetration.
- Substance/Medication-Induced Sexual Dysfunction: Sexual problems caused directly by medication or substance use.
Etiology of Sexual Dysfunctions
Etiology is best understood through a biopsychosocial model, which integrates biological predispositions, psychological factors, and social/relationship influences.
Sexual Dysfunction
Biological Causes
Hormonal Imbalances
- Low testosterone decreases libido
- Hyperprolactinemia suppresses sexual interest
- Thyroid dysfunction affects energy and arousal
Medical Illnesses
Chronic illnesses have strong associations with sexual dysfunctions:
- Diabetes reduces sensation and blood flow
- Heart disease limits arousal due to circulation issues
- Neurological disorders disrupt nerve functioning
Medications
Common offenders include:
- Selective serotonin reuptake inhibitors (SSRIs)
- Antihypertensives
- Antipsychotic medications
Substance Use
- Chronic alcohol use reduces testosterone
- Smoking impairs blood circulation
- Recreational drugs disrupt hormonal balance
Psychological Causes
Anxiety and Performance Fear
Barlow & Durand (2005) highlight that anxiety is one of the strongest psychological predictors of dysfunction.
Instead of focusing on pleasure, individuals monitor performance, leading to failure.
Depression
Depressed individuals report:
- Low libido
- Reduced energy
- Anhedonia (reduced ability to feel pleasure)
Past Trauma
Survivors of sexual abuse may experience:
- Pain
- Fear
- Avoidance of intimacy
- Dissociation
Negative Beliefs
Examples:
- “Sex is sinful.”
- “My body is unattractive.”
- “I must perform perfectly.”
These beliefs interfere with desire and enjoyment.
Treatment of Sexual Dysfunctions
Treatment must be individualized and multidisciplinary.
Psychological and Behavioral Interventions
Sex Therapy
Following the Masters & Johnson model:
- Sensate focus exercises
- Gradual exposure
- Removing performance pressure
These techniques reduce anxiety and enhance intimacy.
Cognitive Behavioral Therapy (CBT)
Targets:
- Negative beliefs
- Catastrophizing
- Performance anxiety
- Body image issues
CBT improves both desire and arousal.
Mindfulness-Based Therapy
Helps individuals focus on sensations rather than intrusive thoughts.
Couples Therapy
Addresses:
- Communication
- Trust issues
- Emotional closeness
In many cases, treating the relationship improves sexual functioning.
Trauma-Informed Therapy
For individuals with sexual trauma histories.
Medical and Pharmacological Treatments
Erectile Disorder
- PDE5 inhibitors (sildenafil, tadalafil)
- Vacuum erection devices
- Penile injections (in severe cases)
Hormone Therapy
- Testosterone replacement for men
- Estrogen therapy for women with menopausal symptoms
Premature Ejaculation Treatment
- SSRIs (off-label)
- Behavioral stop-start methods
- Topical anesthetic creams
Female Arousal Difficulties
- Vaginal lubricants
- Hormonal creams
- Physical therapy for pelvic floor tension
Pain Disorders
- Vaginal dilators
- Pelvic floor physiotherapy
- Pain desensitization techniques
Lifestyle Interventions
- Exercise improves blood circulation and energy
- Adequate sleep regulates mood
- Stress reduction improves arousal
- Avoidance of alcohol and smoking enhances genital blood flow
Prognosis
Sexual dysfunctions are highly treatable. Early identification improves outcomes. A combination of medical and psychological therapies tends to produce the best results. Supportive partners and open communication are essential predictors of recovery.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.).
Andrew, M. (2011). Clinical Psychology: Science, Practice, and Culture (2nd ed.). Sage.
Alloy, L.B., Riskind, J.H., & Manos, M.J. (2005). Abnormal Psychology: Current Perspectives (9th ed.).
Barlow, D.H., & Durand, V.M. (2005). Abnormal Psychology (4th ed.). Brooks/Cole.
Butcher, J.N., Mineka, S., & Hooley, J.M. (2014). Abnormal Psychology (15th ed.). Pearson.
Carson, R.C., Butcher, J.N., Mineka, S., & Hooley, J.M. (2007). Abnormal Psychology (13th ed.). Pearson.
Nevid, J.S., Rathus, S.A., & Greene, B. (2014). Abnormal Psychology (9th ed.). Pearson.
Puri, B.K., Laking, P.J., & Treasaden, I.H. (1996). Textbook of Psychiatry. Churchill Livingstone.
Sarason, I.G., & Sarason, R.B. (2002). Abnormal Psychology: The Problem of Maladaptive Behavior (10th ed.).
WHO. (2019). International Classification of Diseases, ICD-11.
Niwlikar, B. A. (2025, November 28). Sexual Cycle & 8 Important Sexual Dysfunction Disorders: Diagnosis, Causes, and Treatments. Careershodh. https://www.careershodh.com/sexual-cycle-sexual-dysfunction-disorders/