
Introduction
Psychopathology, the scientific study of mental disorders, is shaped by diverse theoretical paradigms that attempt to explain the origin, manifestation, and treatment of abnormal behavior. Each paradigms in psychopathology reflects unique assumptions about human nature, the causes of psychological distress, and appropriate intervention strategies. The importance of paradigms lies not only in their explanatory power but also in how they guide diagnosis, therapy, and research.
The DSM-5 (American Psychiatric Association, 2013) and the ICD-10 (World Health Organization, 1992) are diagnostic systems that adopt an eclectic stance, reflecting insights from multiple paradigms. From the medicalized biological paradigm to the socially informed sociocultural model, these frameworks capture the multifaceted nature of mental illness.

Holistic Model of Pathology
Read More: Psychoanalysis
1. Biological Paradigm
The biological paradigm, often described as the “medical model,” conceptualizes mental disorders as diseases of the brain.
Assumptions and Foundations
- Psychological disorders are caused by neurobiological abnormalities, genetic inheritance, or brain injury.
- Symptoms are considered manifestations of underlying physiological dysfunctions.
Key Evidence
- Neurotransmitters: Dysregulation of serotonin and dopamine is linked to depression and schizophrenia respectively (Butcher, Mineka, & Hooley, 2014).
- Genetics: Twin studies show heritability rates of 40–70% for disorders like bipolar disorder (Carson et al., 2007).
- Brain Structure: Neuroimaging reveals structural differences in conditions such as Alzheimer’s disease.
Treatment Approaches
- Pharmacotherapy: Antidepressants, anxiolytics, and antipsychotics form the core interventions.
- Somatic Treatments: Electroconvulsive therapy (ECT) and, historically, psychosurgery.
While powerful, the model is criticized for reductionism—neglecting psychological and social factors. It risks labeling patients as passive recipients of treatment.
2. Psychoanalytical Paradigm
Founded by Sigmund Freud, the psychoanalytical paradigm emphasizes unconscious processes and childhood experiences.
Assumptions and Mechanisms
- Mental disorders stem from unresolved unconscious conflicts.
- Defense mechanisms such as repression and projection distort reality, leading to maladaptive behavior (Comer, 2007).
Applications
- Anxiety Disorders: Explained as conflicts between the id, ego, and superego.
- Depression: Linked to loss and introjection of anger toward the self (Davison, Neal, & Kring, 2004).
Therapeutic Interventions
- Free Association: Patients verbalize thoughts without censorship.
- Dream Analysis: Interpreting symbolic meanings of dreams.
- Transference Analysis: Understanding unconscious feelings projected onto the therapist.
Psychodynamic Psychotherapy
Psychoanalysis is often faulted for being unscientific and difficult to test empirically. Yet, its emphasis on early experience and unconscious processes has profoundly influenced modern therapy.
3. Behavioristic Paradigm
The behavioristic paradigm posits that abnormal behavior is learned and can therefore be unlearned.
Core Assumptions
- Classical Conditioning: Phobias can develop when neutral stimuli are paired with aversive events (e.g., Little Albert experiment by Watson).
- Operant Conditioning: Maladaptive behaviors are maintained through reinforcement (e.g., compulsive handwashing reduces anxiety, reinforcing the behavior).
- Modeling: Observing and imitating others’ behaviors, as in Bandura’s social learning theory.
Applications
- Phobias: Learned fear responses (e.g., fear of dogs after a bite).
- Substance Abuse: Reinforced by pleasurable effects of substances.
Interventions
- Systematic Desensitization: Gradual exposure to feared stimuli.
- Token Economies: Reinforcement systems in hospitals.
- Aversion Therapy: Pairing maladaptive behavior with unpleasant stimuli.
The paradigm overlooks inner thoughts and emotions, reducing human behavior to stimulus-response patterns (Sue, Sue, & Sue, 2006).
4. Cognitive Paradigm
Emerging as a response to the limitations of behaviorism, the cognitive paradigm emphasizes dysfunctional thought processes.
Core Assumptions
- Abnormal behavior results from maladaptive cognitions—distorted ways of interpreting the world (Nevid, Rathus, & Greene, 2014).
- Schemas and automatic thoughts play a central role.
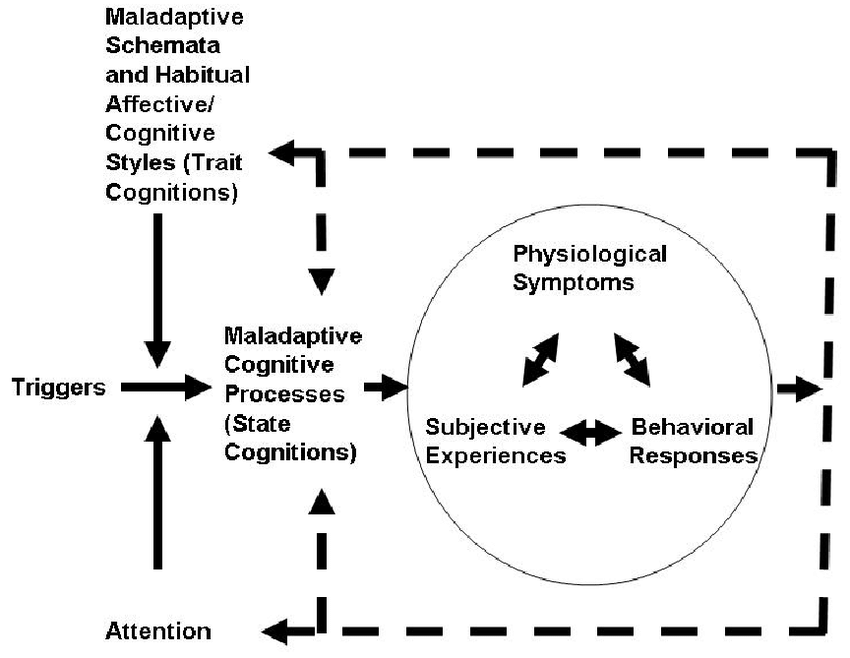
Cognitive Model of Psychopathology
Key Theories
- Aaron Beck’s Cognitive Theory: Depression results from the cognitive triad—negative views of the self, world, and future.
- Albert Ellis’ Rational Emotive Behavior Therapy (REBT): Emotional distress arises from irrational beliefs (e.g., “I must be loved by everyone”).
Treatment
- Cognitive-Behavioral Therapy (CBT): Combines cognitive restructuring with behavioral techniques.
- Mindfulness-Based Approaches: Address cognitive rumination and stress.
Cognitive approaches may underplay emotional and biological factors. Nevertheless, CBT is among the most empirically validated treatments today (Barlow & Durand, 2005).
5. Humanistic-Existential Paradigm
The humanistic-existential paradigm focuses on personal growth, self-actualization, and existential concerns.
Core Assumptions
- Humans are inherently good and strive toward realizing their potential (Nolen-Hoeksema, 2004).
- Psychopathology arises from incongruence between the self-concept and actual experience, or from existential crises (e.g., confronting meaninglessness).
Influential Thinkers
- Carl Rogers: Advocated client-centered therapy with unconditional positive regard.
- Viktor Frankl: Developed logotherapy, emphasizing meaning-making in suffering (e.g., survivors of concentration camps).
Interventions
- Non-Directive Therapy: Encourages self-exploration.
- Existential Therapy: Helps clients confront freedom, isolation, and death.
Critics argue the model lacks empirical rigor and may be too idealistic. However, it emphasizes empathy, authenticity, and dignity—qualities sometimes overlooked in more mechanistic paradigms.
6. Biopsychosocial Paradigm
The biopsychosocial paradigm integrates biological, psychological, and social factors.
Core Assumptions
- Disorders result from the interaction of diathesis (vulnerability) and stressors.
- Vulnerabilities may be genetic, cognitive, or personality-based, while stressors include trauma, poverty, or discrimination (Carson et al., 2007).
Example
- Depression: Genetic predisposition interacts with stressful life events, such as loss or financial hardship.
- Schizophrenia: Environmental triggers (e.g., prenatal exposure to viruses) interact with genetic vulnerability.
Clinical Relevance
This model underpins modern psychiatry and psychology, guiding individualized treatment plans that combine medication, psychotherapy, and social interventions (Alloy, Riskind, & Manos, 2005). The challenge lies in operationalizing and quantifying the exact contributions of each factor. Yet, it remains the dominant paradigm today.
7. Sociocultural Paradigm
The sociocultural paradigm highlights the role of cultural, societal, and environmental factors in psychopathology.
Core Assumptions
- Mental illness cannot be understood in isolation from cultural context (Sue, Sue, & Sue, 2006).
- Poverty, stigma, and systemic discrimination exacerbate vulnerability.
Key Evidence
- Culture-Bound Syndromes: Conditions like koro (anxiety about genital retraction) and ataque de nervios (panic-like episodes in Latin cultures).
- Epidemiology: Rates of depression are higher among marginalized groups facing socioeconomic stressors.
Implications
- Culturally Sensitive Therapy: Incorporating patients’ cultural beliefs into treatment.
- Policy and Advocacy: Addressing social determinants of health through systemic change.
The paradigm may underemphasize individual and biological factors. However, it broadens understanding by situating mental health within a societal framework.
Integration of Paradigms
No single paradigm sufficiently explains psychopathology. Butcher, Mineka, & Hooley (2014) and Alloy et al. (2005) emphasize the growing preference for integrative approaches:
Case Example (PTSD): A soldier develops PTSD after combat. The biological paradigm highlights hyperactive amygdala activity, the cognitive paradigm examines maladaptive beliefs (“I am never safe”), the behavioristic model explains avoidance behavior, while the sociocultural paradigm emphasizes stigma in seeking help. An integrated treatment plan may combine SSRIs, CBT, exposure therapy, and peer support groups.
Such integration reflects the complexity of mental health, ensuring more comprehensive and effective interventions.
Conclusion
The paradigms of psychopathology—biological, psychoanalytical, behavioristic, cognitive, humanistic-existential, biopsychosocial, and sociocultural—offer diverse lenses through which abnormal behavior is understood. Each paradigm contributes unique insights, from the molecular underpinnings of disorders to the sociocultural contexts that shape expression and treatment.
While earlier approaches often competed, contemporary practice acknowledges the value of integration, particularly within the biopsychosocial framework. This paradigm reflects the dynamic interplay of vulnerabilities and environmental stressors, aligning with global diagnostic systems like the DSM-5. Ultimately, the paradigms collectively enrich the science and practice of psychopathology, offering pathways not only for treatment but also for prevention, advocacy, and human understanding.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: APA.
Alloy, L.B., Riskind, J.H., & Manos, M.J. (2005). Abnormal Psychology: Current Perspectives (9th ed.). Tata McGraw-Hill.
Barlow, D.H., & Durand, V.M. (2005). Abnormal psychology (4th ed.). Brooks/Cole.
Butcher, J.N., Mineka, S., & Hooley, J.M. (2014). Abnormal Psychology (15th ed.). Pearson.
Carson, R.C., Butcher, J.N., Mineka, S., & Hooley, J.M. (2007). Abnormal Psychology (13th ed.). Pearson Education.
Comer, R.J. (2007). Abnormal psychology (6th ed.). Worth Publishers.
Davison, G.C., Neal, J.M., & Kring, A.M. (2004). Abnormal psychology (9th ed.). Wiley.
Nevid, J.S., Rathus, S.A., & Greene, B. (2014). Abnormal Psychology (9th ed.). Pearson Education.
Nolen-Hoeksema, S. (2004). Abnormal Psychology (3rd ed.). McGraw-Hill.
Sue, D., Sue, D.W., & Sue, S. (2006). Abnormal behavior (8th ed.). Houghton Mifflin.
World Health Organization. (1992). The ICD-10 Classification of Mental and Behavioral Disorders. Oxford University Press.
Niwlikar, B. A. (2025, September 18). 7 Important Paradigms in Psychopathology. Careershodh. https://www.careershodh.com/paradigms-in-psychopathology/