
Emotional Responses to Chronic Illness – Denial, Anxiety & Depression
Chronic Illness
Healthy people tend to take their health for granted. When a serious illness or injury occurs, their daily activities and social roles are disrupted. Moreover, chronic Illness usually require that patients and their families make permanent behavioral, social, and emotional adjustments.
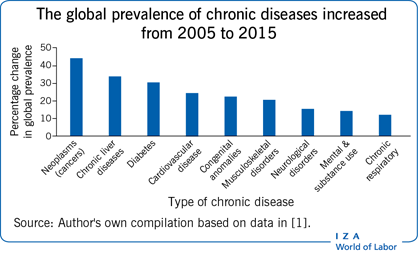
Rise in Chronic Illnesses
Immediately after a chronic illness is diagnosed, a patient can be in a state of crisis marked by physical, social, and psychological disequilibrium. Although, If the patient’s usual coping efforts fail to resolve these problems, the result can be an exaggeration of symptoms and their meaning, indiscriminate eff orts to cope, an increasingly negative attitude, and worsening health (Drossman et al., 2000; Epker & Gatchel, 2000).
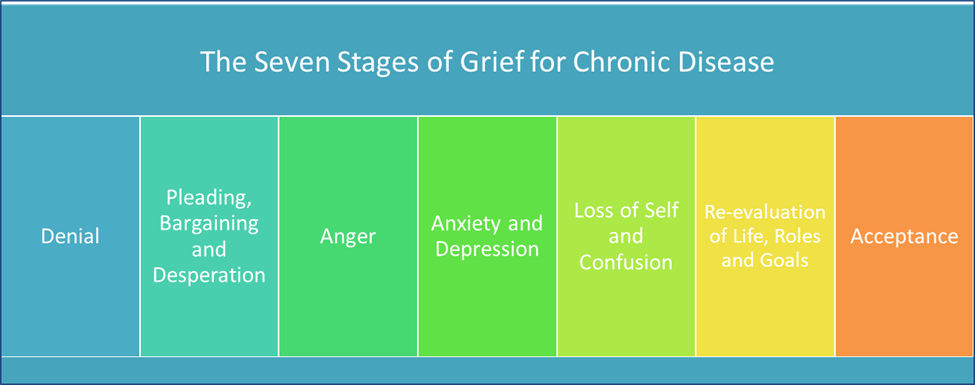
Grief and Chronic Illness
The people who have this chronic health disorder are more likely to suffer from depression, anxiety, and generalized distress (De Graaf & Bijl, 2002; Mittermaier et al., 2004). Moreover, these psychological changes are important because they compromise quality of life, predict adherence to treatment, and increase the risk of dying early (Bruce, Hancock, Arnett, & Lynch, 2010; Christensen, Moran, Wiebe, Ehlers, & Lawton, 2002). So here, we will read about the emotional responses to chronic illness.
Emotional Responses to Chronic Illness
Generally people facing the chronic illness will give following emotional responses.
- Denial
- Anxiety
- Depression
1. Denial
Denial is a defense mechanism by which people avoid the implications of an illness. It is a common early reaction to chronic illness (Krantz & Deckel, 1983; Meyerowitz, 1983). Patients may act as if the illness is not severe, it will shortly go away, or it will have few long-term implications.
Immediately after the diagnosis of illness, denial can serve a protective function by keeping the patient from having to come to terms with problems posed by the illness when he or she is least able to do so (Hackett & Cassem, 1973; Lazarus, 1983).
Over time, however, any benefit of denial gives way to its costs. It can interfere with taking in necessary treatment information and compromise health (Mund & Mitte, 2012).
2. Anxiety
Anxiety is also common. Many patients are overwhelmed by the potential changes in their lives and, in some cases, by the prospect of death. According to Rabin, Ward, Leventhal, & Schmitz, (2001), Anxiety is especially high when people are
- Waiting for test results,
- Receiving diagnoses,
- Awaiting invasive medical procedures, and
- Anticipating or experiencing adverse side effects of treatment.
Anxiety is a problem not only because it is intrinsically distressing but also because it interferes with treatment.
For example,
- Anxious patients cope more poorly with surgery (Mertens, Roukema, Scholtes, & De Vries, 2010);
- Anxious diabetic patients have poor glucose control (Lustman, 1988);
- Anxiety exacerbates sickle cell disease (Levenson et al., 2008),
- Irritable bowel syndrome (Blomhoff , Spetalen, Jacobsen, & Malt, 2001) and
- Multiple sclerosis (Kehler & Hadjistavropoulos, 2009);
- Anxious MI patients are less likely to return to work on schedule (Maeland & Havik, 1987).
- Anxiety is especially prevalent among people with asthma and pulmonary disorders (Katon, Richardson, Lozano, & McCauley, 2004).
- Symptoms of anxiety may also be mistaken for symptoms of the underlying disease and thus interfere with assessments of the disease and its treatment (Chen, Hermann, Rodgers, Oliver-Welker, & Strunk, 2006).
3. Depression (common reaction to chronic illness)
Up to 33% of all medical inpatients with chronic disease report symptoms of depression, and up to 1/4th suffer from severe depression (Moody, McCormick, & Williams, 1990). Depression is especially common among stroke patients, cancer patients, and heart disease patients, as well as among people with more than one chronic disorder (Egede, 2005; see Taylor & Aspinwall, 1990, for a review).
At one time, depression was regarded only as an emotional disorder, but its medical significance is increasingly recognized. However, people who have intermittent bouts of depression are more likely to get heart disease, atherosclerosis, hypertension, stroke, dementia, osteoporosis, and Type II diabetes, and at younger ages. Moreover, depression exacerbates the course of several chronic disorders, most notably coronary heart disease.
Although, depression complicates treatment adherence and medical decision making. As a result, It interferes with patients adopting a comanagerial role, and it leads to enhanced risk of mortality from several chronic diseases (Novak et al., 2010; van Dijk et al., 2012).

Chronic Illness and Depression
Depression is sometimes a delayed reaction to chronic illness, because it takes time for patients to understand the full implications of their condition.
Assessing Depression
Depression is so prevalent among chronically ill patients that experts recommend routine screening for depressive symptoms during medical visits. Although, many symptoms of depression- fatigue, sleeplessness, and weight loss, can also be symptoms of disease or side effects of a treatment.
If depressive symptoms are because of illness or treatment, their significance may be less apparent, and, consequently, depression might not need aby treatment (Ziegelstein et al., 2005).
Symptoms of anxiety may also be mistaken for symptoms of the underlying disease. As a result, it interfere with assessments of the disease and its treatment (Chen, Hermann, Rodgers, Oliver-Welker, & Strunk, 2006).
Who Gets Depressed?
- Depression increases with the severity of the illness (Cassileth et al., 1985; Moody et al.,1990)
- Depression increases with pain and disability (Turner & Noh, 1988; Wulsin, Vaillant, & Wells, 1999).
- Who are experiencing other negative life events and lack of social support (Bukberg, Penman, & Holland, 1984; Thompson et al., 1989).
It is important for us to know the emotional responses to chronic illness.
Read More- Coping Mechanism to Stress
References
Taylor, Shelley E. (2018). Health Psychology (10th ed). McGraw Hill Higher Education. Indian Edition
Niwlikar, B. A. (2022, February 9). 3 Important Emotional Responses to Chronic Illness. Careershodh. https://www.careershodh.com/emotional-responses-to-chronic-illness/