
Introduction
Anxiety is a normal human emotion that serves as a survival mechanism, preparing the body to respond to potential threats through the “fight or flight” response. However, anxiety disorders are distinguished from normal anxiety by their intensity, persistence, and the degree to which they interfere with an individual’s daily functioning (APA, 2013). According to epidemiological studies, anxiety disorders are among the most prevalent psychiatric conditions worldwide, affecting approximately 18% of adults annually and often co-occurring with depression and other psychiatric disorders (Barlow & Durand, 2005).
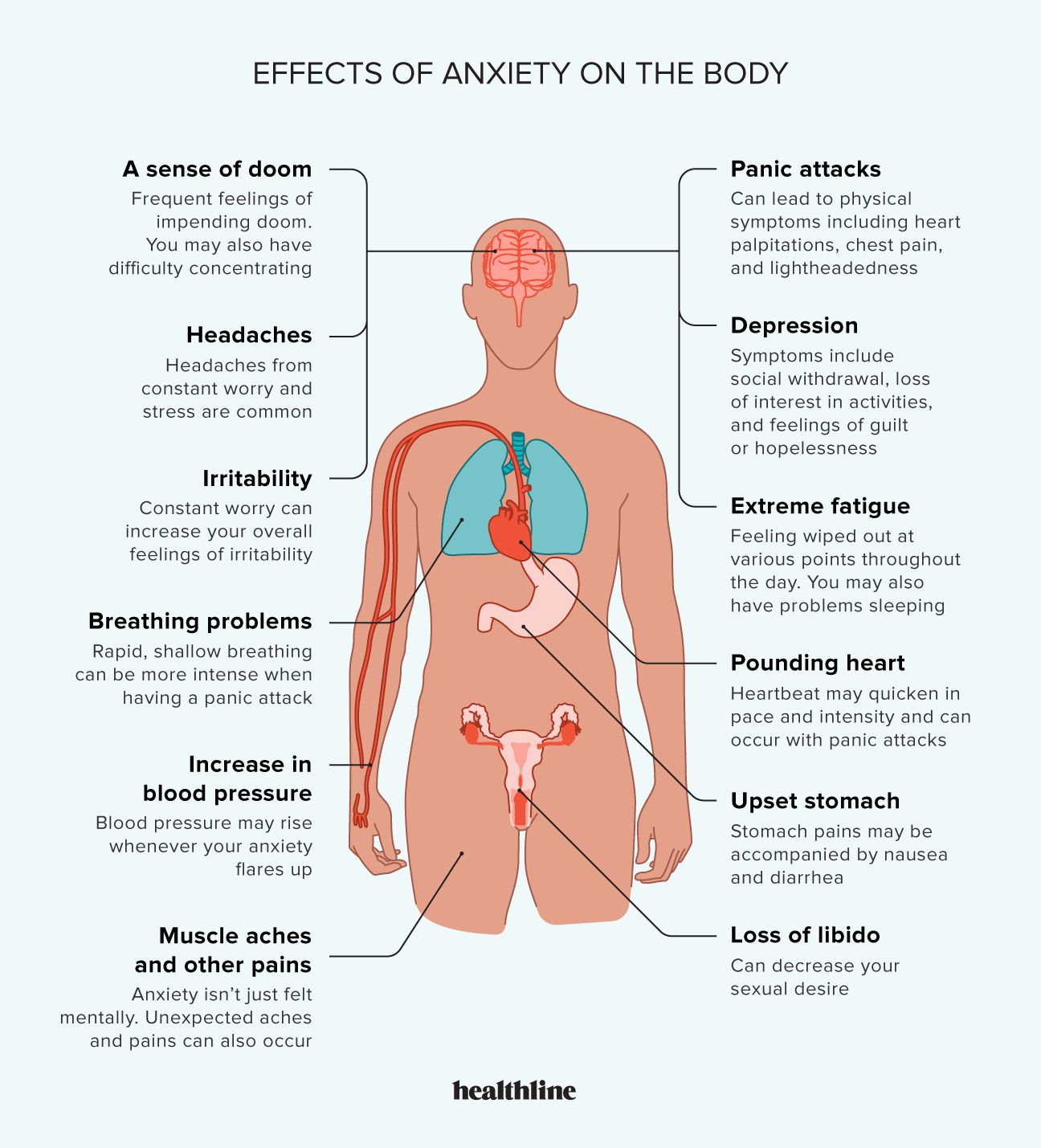
Effects of Anxiety on the Body
The DSM-5 classifies several anxiety disorders, each with distinct features, including Separation Anxiety Disorder, Phobias, Panic Disorder, Generalized Anxiety Disorder (GAD), and Social Anxiety Disorder (SAD). Understanding these disorders requires a multi-dimensional approach involving classification, symptomatology, etiology, and evidence-based treatment.
Read More: DSM vs ICD

Types of Anxiety Disorders
1. Separation Anxiety Disorder (SAD)
Separation Anxiety Disorder, once thought to be exclusively a childhood disorder, is now recognized to occur across the lifespan (APA, 2013). It is characterized by excessive anxiety concerning separation from attachment figures, typically parents or primary caregivers. Key diagnostic criteria include:
- Persistent worry about losing attachment figures or experiencing harm to them.
- Reluctance or refusal to leave home or go to school due to fear of separation.
- Recurrent nightmares involving separation.
- Physical complaints, such as headaches, nausea, or stomachaches, during anticipated separation.
Symptoms must last at least four weeks in children and six months in adults and cause significant impairment in social, academic, or occupational functioning.
Example: A 10-year-old child becomes physically ill every time school starts and cannot attend without the presence of a parent, demonstrating the core features of SAD.
Epidemiology
SAD is common in childhood, with prevalence rates ranging from 4–5%, and often coexists with other anxiety disorders, depression, and somatic complaints. Adult SAD is less frequent but can result in persistent functional impairment, particularly in social and occupational domains (Nevid, Rathus, & Greene, 2014).
Etiology
The etiology of SAD is multifactorial:
- Genetic factors: Twin and family studies indicate moderate heritability (Barlow & Durand, 2005).
- Attachment theory: Insecure or disorganized early attachments increase vulnerability. Children lacking consistent caregiver support may develop heightened separation anxiety (Andrew, 2011).
- Environmental stressors: Traumatic events such as parental divorce, relocation, or loss of a loved one can precipitate SAD (Alloy, Riskind, & Manos, 2005).
- Temperamental factors: Behavioral inhibition in early childhood predisposes individuals to SAD (Butcher, Mineka, & Hooley, 2014).
Treatment
- Cognitive-Behavioral Therapy (CBT): Focuses on graded exposure to separation, cognitive restructuring of catastrophic thoughts, and teaching coping skills (Carson et al., 2007).
- Pharmacotherapy: SSRIs, such as fluoxetine or sertraline, may be prescribed in severe or treatment-resistant cases (APA, 2013).
- Family therapy: Involves educating parents on supportive strategies and gradually reducing overprotective behaviors (Nevid et al., 2014).
Example of therapy: A child may start by staying alone for a few minutes at home, gradually increasing the duration under supervision, paired with positive reinforcement.
2. Phobias
Phobias are intense, irrational fears triggered by specific objects, situations, or activities. The DSM-5 identifies:
- Specific Phobia: Fear of discrete objects (animals, heights, blood).
- Social Anxiety Disorder (Social Phobia): Anxiety about social evaluation or performance.
- Agoraphobia: Fear of situations where escape might be difficult or help unavailable.
Specific phobias are the most common, with lifetime prevalence estimates of 7–9%, while social phobia affects 6–12% of the population (Comer, 2007).
Etiology
- Biological factors: Genetic predisposition and hyperactivity of the amygdala, which regulates fear response (Barlow & Durand, 2005).
- Learning theories: Classical conditioning (e.g., traumatic encounter with a dog leading to cynophobia), and observational learning (modeling) contribute to phobia development.
- Cognitive factors: Catastrophic thinking and overestimation of threat reinforce fear behaviors (Andrew, 2011).
Treatment
- Behavioral therapy: Systematic desensitization and graduated exposure are highly effective.
- Cognitive restructuring: Modifies distorted beliefs about danger and self-efficacy.
- Pharmacotherapy: SSRIs or benzodiazepines may be used for severe anxiety, though psychotherapy is first-line (Davison et al., 2004).
Example: Exposure therapy for a spider phobia may begin with viewing pictures of spiders, progressing to being in the same room as a spider, and eventually handling one under supervision.
3. Panic Disorder
Panic Disorder involves recurrent, unexpected panic attacks—intense surges of fear with somatic and cognitive symptoms. Panic attacks peak within minutes and may include:
- Palpitations or tachycardia
- Shortness of breath
- Dizziness or lightheadedness
- Derealization or depersonalization
The disorder is diagnosed when attacks are followed by at least one month of persistent concern or behavior change (APA, 2013). Agoraphobia is often comorbid.

Panic Cycle
Epidemiology
Lifetime prevalence is 2–5%, more common in women. Onset typically occurs in late adolescence or early adulthood (Butcher et al., 2014).
Etiology
- Biological factors: Dysregulation of neurotransmitters (serotonin, norepinephrine) and hypersensitive autonomic nervous system.
- Cognitive theories: Catastrophic misinterpretation of bodily sensations leads to a vicious cycle of panic (Barlow & Durand, 2005).
- Environmental factors: Stressful life events, such as loss, trauma, or major transitions, may precipitate panic attacks (Andrew, 2011).
Treatment
- CBT: Interoceptive exposure, cognitive restructuring, and relaxation training.
- Pharmacotherapy: SSRIs (e.g., paroxetine) and benzodiazepines for acute management.
- Lifestyle management: Regular exercise, avoidance of caffeine, and mindfulness techniques (Carson et al., 2007).
4. Generalized Anxiety Disorder (GAD)
GAD is defined by excessive, uncontrollable worry about multiple domains, lasting at least six months (APA, 2013). Associated symptoms include:
- Restlessness or feeling keyed up
- Fatigue
- Difficulty concentrating
- Irritability
- Muscle tension
- Sleep disturbances
Symptoms cause significant impairment in daily life.
Epidemiology
GAD affects 3–6% of the population, with higher rates in women. It frequently co-occurs with depression, panic disorder, and substance use disorders (Nevid et al., 2014).
Etiology
- Genetic and neurobiological factors: Deficits in GABAergic and serotonergic systems, hyperactive amygdala.
- Cognitive factors: Dysfunctional worry patterns, intolerance of uncertainty (Comer, 2007).
- Environmental stressors: Chronic stress, trauma, and early childhood adversity (Alloy et al., 2005).
Treatment
- CBT: Focuses on cognitive restructuring, exposure to worry, relaxation techniques.
- Pharmacotherapy: SSRIs, SNRIs, and buspirone are effective first-line treatments.
- Complementary interventions: Mindfulness meditation, yoga, and stress management enhance outcomes (Barlow & Durand, 2005).
5. Social Anxiety Disorder (SAD)
SAD is characterized by fear or anxiety about social situations where the individual may be scrutinized. Symptoms include:
- Avoidance of social interactions
- Physical manifestations (blushing, sweating, trembling)
- Fear of embarrassment or humiliation
- Anticipatory anxiety prior to social events
Onset usually occurs in adolescence, with significant impact on education, work, and relationships (APA, 2013).
Etiology
- Genetic factors: High heritability; family studies show clustering of social anxiety (Butcher et al., 2014).
- Neurobiological factors: Hyperactive amygdala and hypoactive prefrontal regulation of fear responses.
- Cognitive factors: Negative self-perception and exaggerated fear of negative evaluation (Andrew, 2011).
- Environmental factors: Early social rejection, bullying, or overprotective parenting (Alloy et al., 2005).
Treatment
- CBT: Exposure therapy, cognitive restructuring, and social skills training.
- Pharmacotherapy: SSRIs, sometimes beta-blockers for performance anxiety.
- Group therapy: Provides a controlled environment for social exposure (Carson et al., 2007).
Conclusion
Anxiety disorders, including Separation Anxiety, Phobias, Panic Disorder, GAD, and Social Anxiety Disorder, are complex, multifactorial conditions affecting millions worldwide. Etiology involves interactions among genetic, neurobiological, cognitive, and environmental factors. Treatments are evidence-based, combining psychotherapy, pharmacotherapy, and lifestyle interventions. Early recognition and intervention are crucial to improving prognosis and functional outcomes. Future research should focus on personalized treatment approaches and preventive strategies to reduce the global burden of anxiety disorders.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Arlington, VA: American Psychiatric Association.
Andrew, M. (2011). Clinical psychology: Science, practice, and culture (2nd Edn). Sage Publication.
Alloy, L.B., Riskind, J.H., & Manos, M.J. (2005). Abnormal Psychology: Current perspectives (9th Edn). Tata McGraw-Hill.
Barlow, D.H., & Durand, V.M. (2005). Abnormal psychology (4th ed.). Pacific Grove: Books/Cole.
Butcher, J.N., Mineka, S., & Hooley, J.M. (2014). Abnormal Psychology (15th Ed.). Dorling Kindersley (India) Pvt. Ltd.
Carson, R.C., Butcher, J.N., Mineka, S., & Hooley, J.M. (2007). Abnormal Psychology (13th Edn). Pearson Education, India.
Comer, R.J. (2007). Abnormal Psychology (6th ed.). New York: Worth Publishers.
Davison, G.C., Neal, J.M., & Kring, A.M. (2004). Abnormal Psychology (9th ed.). New York: Wiley.
Nevid, J.S., Rathus, S.A., & Greene, B. (2014). Abnormal Psychology (9th Edn). Pearson Education.
Nolen-Hoeksema, S. (2004). Abnormal Psychology (3rd Edn). McGraw-Hill.
Niwlikar, B. A. (2025, September 26). 5 Important Types of Anxiety Disorders: Classifications, Types, Etiology, and Treatments. Careershodh. https://www.careershodh.com/types-of-anxiety-disorders/