
Introduction
Emotion-Focused Therapy (EFT) and Lazarus’s Multimodal Therapy (MMT) represent two major contemporary orientations in counseling and psychotherapy. Although they differ significantly in their theoretical assumptions and clinical strategies, both approaches reflect broad trends in counseling psychology: an integrative, evidence-informed, and client-centered practice (Gelso & Williams, 2022). EFT emerged from humanistic and experiential psychotherapy traditions, focusing on the transformation of emotional processes. In contrast, Multimodal Therapy, developed by Arnold Lazarus, is grounded in social-learning and cognitive-behavioral traditions and emphasizes comprehensive, individualized intervention across multiple modalities of functioning.
Read More: Psychodynamic
1. Emotion-Focused Therapy (EFT)
Emotion-Focused Therapy was formally developed by Leslie Greenberg and colleagues in the 1980s. Although Greenberg’s work is not part of the sources you provided, the tradition behind EFT—humanistic-experiential therapy—draws heavily on the work of Rogers, Perls, and Gendlin, all of whom are widely cited in counseling psychology texts (Corey, 2008; Feltham & Horton, 2006). EFT blends humanistic principles (empathy, authenticity, unconditional acceptance) with process-experiential methods.

Stages of Emotionally Focused Therapy
Humanistic Roots
Humanistic counseling, strongly represented in counseling psychology (Gelso & Williams, 2022), emphasizes:
The actualizing tendency
Experiential awareness
Therapist presence
Emotional expression as central to growth
EFT extends this tradition by asserting that maladaptive emotional schemes underlie psychological distress and that transforming these emotional structures—rather than merely understanding or controlling them—creates therapeutic change.
View of Human Nature
EFT conceptualizes humans as inherently growth-oriented, capable of self-enhancement, and wired for emotional intelligence (Feltham & Horton, 2006). Emotions are not obstacles but fundamental adaptive processes that provide information, guide decision-making, and motivate behavior. This is consistent with modern counseling psychology’s emphasis on strengths, resilience, and client resources (Gelso & Williams, 2022).
Core Concepts
Some core concepts include, the following:
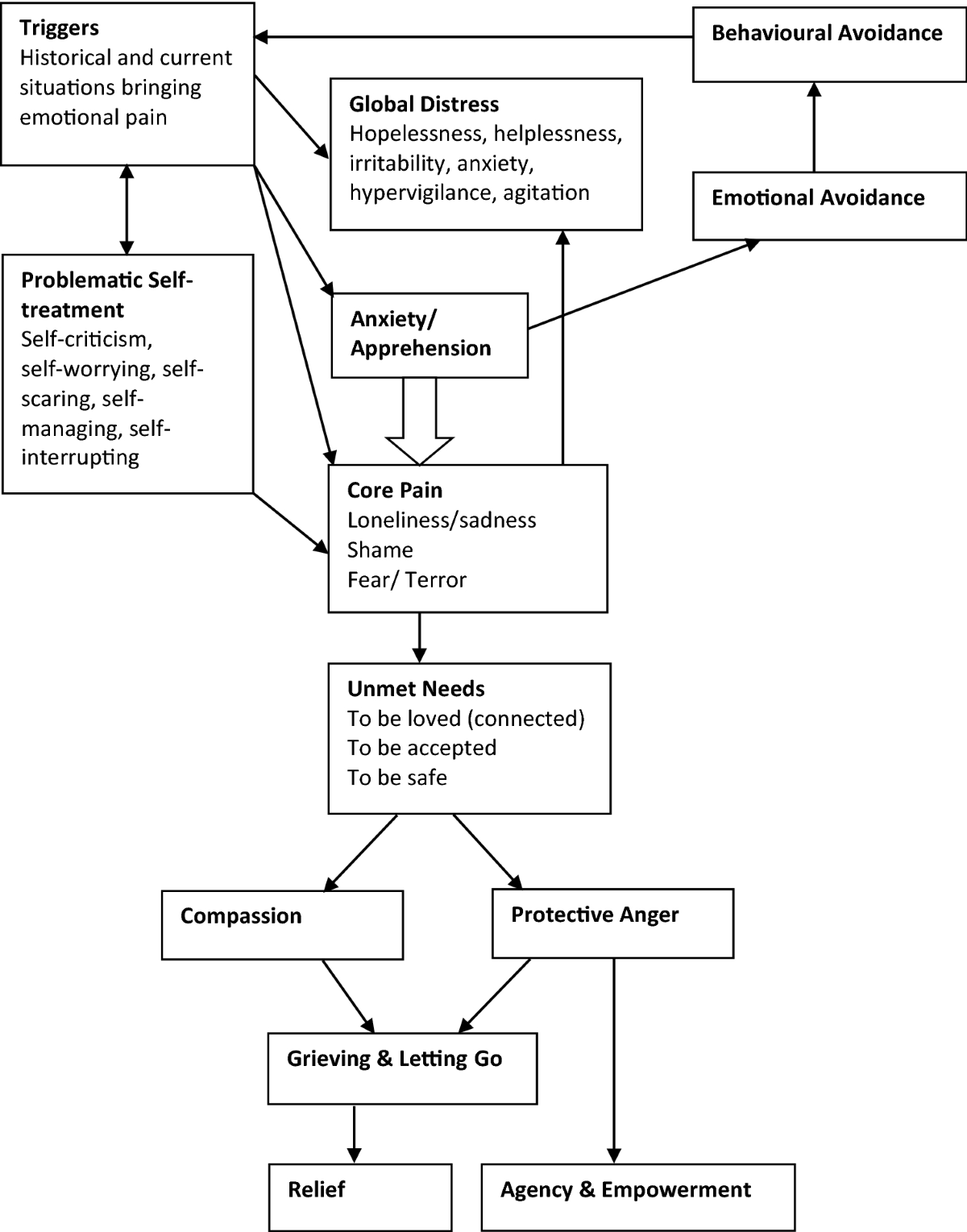
1. Emotion Schemes
EFT posits that clients carry emotional memories and patterns—“schemes”—formed through past experiences. These influence how individuals interpret events, relationships, and internal states.
2. Primary vs. Secondary Emotions
Primary Adaptive Emotions: healthy, direct responses (e.g., grief after loss)
Primary Maladaptive Emotions: maladaptive, often trauma-based emotions (e.g., shame from childhood abuse)
Secondary Emotions: defenses or reactions to primary emotions (e.g., anger covering sadness)
Therapy aims to transform primary maladaptive emotions into adaptive ones.
3. Experiential Processing
Clients are guided to access, symbolize, process, and transform emotional experiences through in-session techniques such as chair-work and focusing.
Therapeutic Relationship
The therapeutic relationship in EFT is essential. Humanistic foundations emphasize:
Empathic attunement
Genuineness
Non-judgment
Presence
Gelso & Williams (2022) argue that therapeutic relationships serve both a healing and a working function, consistent with EFT’s reliance on relational depth.
Goals of EFT
Increase emotional awareness
Transform maladaptive emotions
Strengthen emotion regulation
Resolve internal conflicts
Promote healthier interpersonal patterns
The goal is not simply to cathartically express emotion but to reorganize emotional meaning structures.
Emotion-Focused Therapy
Therapeutic Techniques
Although Greenberg’s original techniques are specific, the general experiential methods are widely discussed in psychotherapy literature:
1. Two-Chair Work
Clients enact conflicting parts of the self (e.g., self-criticism vs. vulnerability) in dialogue to facilitate integration.
2. Empty-Chair Work
Adapted from Gestalt therapy, this technique allows clients to express unfinished feelings toward significant others.
3. Focusing
Clients attend to bodily felt senses to access implicit emotional knowledge.
4. Empathic Exploration
The therapist facilitates deepening awareness and reflection.
Corey (2008) notes that experiential methods like chair-work have proven effective in groups as well, helping individuals confront internal conflicts in a supportive environment.
Multicultural Considerations
Feltham & Horton (2006) and Woolfe & Dryden (1996) emphasize that experiential therapies must adapt to cultural norms regarding emotional expression. Some clients may come from traditions that value emotional restraint or collective harmony. Therefore, EFT must be adjusted to avoid imposing Western emotional norms.
Strengths of EFT
Emphasizes emotional depth and authenticity
Supported by empirical evidence (not in your sources but widely recognized)
Integrates well with other modalities
Offers a clear process of change
Aligns with humanistic values highlighted in counseling psychology literature (Gelso & Williams, 2022)
Criticisms of EFT
Emotion-focused work may overwhelm some clients, especially those with trauma or unstable functioning (Feltham & Horton, 2006).
Less structured than cognitive-behavioral approaches, potentially challenging for highly anxious clients.
Cultural mismatch for clients who prefer problem-solving or cognitive interventions.
Emotion-intensity may risk dependency if not balanced with skill-building.
2. Lazarus’s Multimodal Therapy (MMT)
Developed by Arnold Lazarus, MMT is an extension of behavioral therapy but reframed within a multimodal, holistic framework. Lazarus argued that effective therapy must address multiple dimensions of human functioning rather than a single theoretical lens.
Rimm & Masters (1987), reviewing behavioral therapies, note that Lazarus played a central role in broadening behavior therapy beyond pure conditioning into a more integrative, skills-based model.
Theoretical Foundations
MMT emphasizes that humans function across multiple, interrelated domains. Treatment must therefore be individually tailored and assessment-driven. MMT is grounded in:
Social learning theory
Cognitive-behavioral principles
Technical eclecticism
It aligns with Prochaska & Norcross’s (2007) description of psychotherapy systems evolving toward integrative practice.
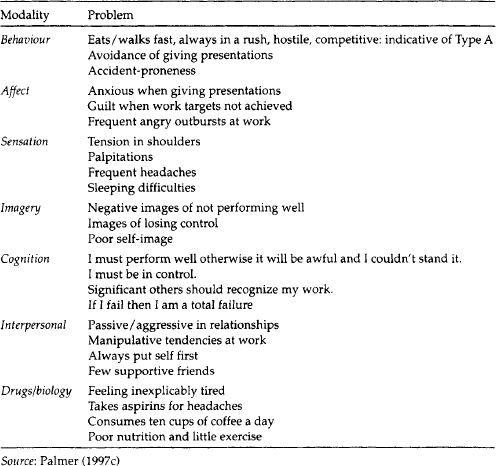
The BASIC-ID Assessment System
Lazarus proposed that human functioning can be understood through seven modalities, remembered through the acronym BASIC-ID:
B – Behavior: actions, habits
A – Affect: emotions
S – Sensation: bodily responses
I – Imagery: internal visualizations
C – Cognition: thoughts, beliefs
I – Interpersonal: relationships
D – Drugs/Biology: physical health, medication
This multidimensional framework allows therapists to construct a comprehensive individualized treatment plan.
Multimodal Therapies
View of Human Nature
MMT assumes that human behavior is influenced by interaction between biological, psychological, and social-learning factors (Capuzzi & Gross, 2008). Unlike singular theories, MMT rejects the idea that any one aspect of functioning dominates.
The approach aligns with contemporary counseling psychology, which supports integrative, biopsychosocial thinking (Gelso & Williams, 2022).
Clinical Goals
Provide a comprehensive assessment of the client’s functioning
Formulate an individualized treatment plan
Target each relevant modality with specific interventions
Build coping strategies across modalities
Promote long-term behavioral change
Techniques in Multimodal Therapy
Because MMT is technically eclectic, interventions vary widely and may include:
1. Behavioral Techniques
Reinforcement, contingency management, exposure, skills training (Rimm & Masters, 1987).
2. Cognitive Techniques
CBT-style restructuring of beliefs (Beck, 1976).
3. Affective/Emotion Regulation Approaches
Relaxation, mindfulness, imagery.
4. Sensory/Physiological Methods
Biofeedback, exercise recommendations, desensitization.
5. Interpersonal Training
Assertiveness training, communication skills (Corey, 2008).
6. Imagery-Based Techniques
Guided imagery to modify internal representations.
7. Biological/Health-Based Interventions
Medication consultations, sleep hygiene, nutritional considerations.
Lazarus insisted that techniques must be selected empirically and pragmatically, not ideologically—an early form of evidence-informed practice.
Therapeutic Relationship in MMT
While MMT is technique-driven, Lazarus emphasized a firm, supportive, and honest therapeutic stance. The rapport is not as central as in EFT, but effective collaboration remains important.
Gelso & Williams (2022) note that even in technically eclectic approaches, the working alliance plays a significant role in outcomes.
Applications of MMT
MMT is widely applicable, especially in:
Anxiety disorders
Depression
Addictive behaviors
Stress management
Somatic concerns
Interpersonal difficulties
Because the model is highly adaptive, it suits clients who prefer structured, goal-oriented therapy.
Multicultural Considerations
Feltham & Horton (2006) argue that the BASIC-ID model is flexible enough to incorporate cultural variables such as family norms, bodily expression, cognitive patterns, and community expectations. MMT can be easily adapted for collectivistic, spiritual, or culturally diverse contexts (Veereshwar, 2002; Rama et al., 1976), especially when counselors incorporate culturally specific modalities into assessment and planning.
Strengths of MMT
Highly individualized, avoiding one-size-fits-all treatment.
Integrative and flexible, drawing from many theoretical traditions.
Compatible with evidence-based practice (Prochaska & Norcross, 2007).
Comprehensive assessment through BASIC-ID.
Addresses biological, interpersonal, and lifestyle factors, consistent with modern health psychology.
Criticisms of MMT
Complexity: Requires high clinical skill to integrate many techniques.
Risk of theoretical incoherence: Critics argue that eclecticism can lack philosophical unity (Feltham & Horton, 2006).
Time-consuming assessment: BASIC-ID requires detailed exploration.
Technique overload: Therapists may rely too heavily on interventions rather than depth processes.
Potential superficiality: Some argue that focusing on multiple modalities may overlook deeper psychological or emotional themes (Corsini & Wedding, 1995).
Conclusion
Emotion-Focused Therapy and Multimodal Therapy exemplify two major but distinct paths within modern counseling psychology. EFT continues the humanistic-experiential tradition, emphasizing emotional transformation, depth, and relational attunement. In contrast, Multimodal Therapy represents an integrative, assessment-driven approach grounded in behavioral and cognitive science.
Both approaches reflect the broader movement in counseling toward integrated, client-centered, culturally responsive practice (Gelso & Williams, 2022). EFT contributes a deep understanding of emotion as a pathway to psychological change, while MMT brings a structured, evidence-informed framework for addressing the diverse dimensions of human functioning. Together, they illustrate how counseling psychology values both depth and breadth, both experience and action, both emotion and behavior.
References
Ajaya, S. (1989). Psychotherapy: East and West. Himalayan International Institute.
Beck, A. T. (1976). Cognitive therapy and behavior disorders.
Brown, C., & Augusta-Scott, T. (2007). Narrative therapy. Sage.
Capuzzi, D., & Gross, D. R. (2008). Counseling and psychotherapy: Theories and interventions (4th ed.). Pearson.
Corey, G. (2008). Theory and practice of group counseling. Brooks/Cole.
Corsini, R. J., & Wedding, D. (1995). Current psychotherapies. Peacock.
Ellis, A., & Harper, A. (1975). A new guide to rational living. Prentice-Hall.
Feltham, C., & Horton, I. (2006). The Sage handbook of counselling and psychotherapy (2nd ed.). Sage.
Gelso, C. J., & Fretz, B. R. (1995). Counseling psychology. Prism Books.
Gelso, C. J., & Williams, E. N. (2022). Counseling psychology. American Psychological Association.
Nelson-Jones, R. (2009). Theory and practice of counselling and therapy (4th ed.). Sage.
Prochaska, J. O., & Norcross, J. C. (2007). Systems of psychotherapy: A transtheoretical analysis (6th ed.). Brooks/Cole.
Rama, S., Ballentine, R., & Ajaya, S. (1976). Yoga and psychotherapy. Himalayan International Institute.
Rimm, D. C., & Masters, J. C. (1987). Behavior therapy: Techniques and empirical findings. Harcourt Brace Jovanovich.
Stewart, I. (2000). Transactional analysis counseling in action. Sage.
Veereshwar, P. (2002). Indian systems of psychotherapy. Kalpaz Publications.
Verma, L. (1990). The management of children with emotional and behavioral difficulties. Routledge.
Watts, A. W. (1973). Psychotherapy: East and West. Penguin.
Woolfe, R., & Dryden, W. (1996). Handbook of counseling psychology. Sage.
Niwlikar, B. A. (2025, November 20). 2 important Contemporary Orientations: Emotion-Focused Therapy and Lazarus Multimodal Therapy. Careershodh. https://www.careershodh.com/contemporary-orientations/